The Area Partnership Forum (APF) serves as a pivotal platform for collaborative decision-making and strategic planning within NHS Greater Glasgow and Clyde.
Its primary role is where the NHS Board and 14 recognised Trade Union and professional organisations work together to improve health services for the population of Greater Glasgow and Clyde, and to engage in negotiations with the aspiration of making NHSGGC an exemplar employer.
The Area Partnership Forum will be a powerful enabling force to:
Inform thinking around priorities on health issues.
Inform and test delivery and implementation plans in relation to national strategies.
Advise on workforce planning and development.
Advise on the delivery of the staff governance legislation.
Promote equality and diversity.
Promote and Engage in Partnership Working.
Providing a structured environment for dialogue, the Forum ensures that all voices are heard and contributing to the formulation of policies that reflect the collective interests of the community. The remit of the Area Partnership Forum includes identifying priorities, allocating resources effectively, monitoring progress, and evaluating outcomes to ensure continuous improvement. By promoting transparency, accountability, and inclusivity, the Area Partnership Forum plays a crucial role in driving sustainable development, and improving the quality of life for residents within the area.
Forum meetings are divided between meetings concerned with a broad strategic agenda and those with an agenda constructed around matters more specific to employee relations. Meetings are Co-Chaired by the Chief Executive, Employee Director and the Director of Human Resources and Organisational Development. The Forum provides formal reports to the Staff Governance Committee of the NHS Board.
Civility Saves Lives (CSL) is about how we treat each other at work. The CSL campaign aims to promote positive working relationships and raise awareness about how our behaviour with colleagues can have a direct impact on patient care and outcomes, and staff experience and wellbeing.
It is the responsibility of us all to work together and make conscious decisions about how we behave, so that everyone feels respected, valued, supported and empowered to carry out their work.
The campaign is grounded in research showing that even small acts of rudeness can significantly impact staff wellbeing, team performance, and patient safety.
You can contact your local Organisational Development Advisor to discuss or find out a bit more or visit our SharePoint where you can see the list of groups, contacts, Leads, and watch information videos and download copies of posters.
This year, NHSGGC is celebrating World Kindness Day on Thursday 13 November!
We encourage you to get involved on the day, either by visiting stalls or attending events at your site (more information coming soon!), celebrating with colleagues, or even just making time for a cup of tea and a chat.
This year the Chair, Dr Lesley Thomson KC, presented the Chair’s Awards of Excellence which recognise outstanding achievement, expertise and dedication in patient care. As with all our awards, they celebrate the incredible efforts of our wonderful staff.
The Celebrating Success Event was held on Wednesday 28th May 2025.
The winners were announced live on the night on our social media channels (follow the #ggcawards tag).
You can find out who the winners were and also view their photos and videos below.
Congratulations to all our winners!
Chair Award of Excellence Winner – The Fetal-Genetics Group at the Queen Elizabeth University Hospital
The Fetal-Genetics Group at the Queen Elizabeth University Hospital has been established to improve the experience for patients and families planning or undergoing a pregnancy where there is a known family history of a genetic condition and/or pregnancy loss.
The Fetal-Genetics Group combines the skills of Consultant Obstetricians, Specialist Midwives, Consultant Geneticists, Genetic Counsellors and Clinical Scientists to provide a truly multi-disciplinary approach that allows the most appropriate support and information and any genetic testing to be made available to this group of patients at the earliest opportunity and throughout their pregnancy and beyond.
Chief Executive Award of Excellence Winner – Scottish Epilepsy Register
The Scottish Epilepsy Register has been developed under the leadership of NHSGGC Consultant Neurologist Dr Craig Heath and Johnathan Todd, Head of Information Management. Epilepsy is one of the most common neurological conditions, with an estimated 55,000 people living with it in Scotland. The Scottish Epilepsy Register uses routine health data, collected via a clinical dashboard, to provide an alert to healthcare professionals following a key adverse event. Its main aim is to reduce excessive mortality and morbidity in epilepsy and to improve access to care and outcomes in people living with the condition.
As part of the project, key pieces of clinical information are collected from other health boards which will be used to create a Scottish National Audit Programme for Epilepsy, allowing trends and outcomes to be tracked and monitored. Once fully established, the methodology could be applied to other chronic neurological diseases to improve disease recognition and management.
Was this helpful?
Yes
No
Thanks for your feedback!
The William Cullen Prize for Excellence In Teaching and the William Cullen Prize for Service Innovation are awarded in collaboration with the Royal College of Physicians in Edinburgh.
The Celebrating Success Event was held on 28th May 2025.
The winners were announced live on the night on our social media channels (follow the #ggcawards tag).
You can find out who the winners were and also view their photos and videos below.
Congratulations to all our winners!
William Cullen Prize for Innovation Winner – Red Star Fracture Liaison Service based in the South Sector, led by Dr Maria Talla
The Fracture Liaison Service (FLS) aims to identify and treat patients over the age of 50 who have sustained a fragility fracture, and refer them for an assessment of their bone health in order to reduce their risk of subsequent fractures.
Dr Talla and her team have partnered with RedStar to develop a web-based clinician dashboard system known as RedStar FLS.
The dashboard has significantly reduced the time it takes for the Fracture Liaison Service to identify a patient who has had a fragility fracture, from an average of 15 months to 3 days. This allows prompt assessment and treatment initiation. An automated audit tool has been built into the dashboard and shows that the NHS GGC South Sector FLS is outperforming national FLS standards across the UK.
William Cullen Prize for Education Winner – Intensive Care Medicine in the Glasgow Royal Infirmary
Over the last year, this department has demonstrated an excellent profile in training all grades of doctors, from Foundation to Specialty resident doctors, and has been recognised in providing this in the Scottish Trainee Survey.
The department led by Dr Barbara Miles and her team performs well in many domains, and in particular in important areas such as induction and handover, creating a positive educational environment that is clearly appreciated by the doctors who work there. There is a focus on learning through weekly MDT simulation scenarios and structured learning is provided in weekly education slots on site that can also be accessed remotely.
Was this helpful?
Yes
No
Thanks for your feedback!
Our dedicated teams and individuals were nominated for the prestigious NHSGGC Excellence Awards by patients, visitors and staff. All of our staff have gone above and beyond in the past year and we asked to hear about your experience of outstanding care and for your nominations.
There are 7 categories in our Excellence Awards and the winners were announced at the Celebrating Success Event on 28 May 2025.
The winners were announced live on the night on our social media channels (follow the #ggcawards tag).
You can find out who the Gold Winners were, read about the Silver Winners who were shortlisted, and also view photos and videos in each of the categories below.
Congratulations to all our winners!
Better Care
This award recognises staff who provide and contribute towards incredible patient care improving everyday practices across NHSGGC.
Nominees
Cancer Older People’s service
The Cancer Older Peoples Service at the Beatson has successfully established and implemented a comprehensive Occupational Therapy service which is specifically designed to support older cancer patients. It is the only service of its kind in Scotland and uses targeted interventions to significantly improve functional outcomes for patients, as well as supporting their health and wellbeing. The team also concentrates on ensuring safe discharge for patients from hospital, and the best ways to avoid unnecessary hospital admissions. They will undertake a thorough assessment of a patient’s physical, psychological, and social needs, while also incorporating age-specific screenings and interventions into routine cancer care.
Evaluation has shown positive improvements in clinical outcomes, patient satisfaction, and overall cost-effectiveness, with clear areas identified for further growth. The team is currently in discussion with other cancer centres across the country to share its framework, which has proven to be a highly transferable model.
Charley Mcdowall – Transition clinic within Inverclyde CAMHS
Charley is a specialist mental health nurse working in the Child and Adolescent Mental Health Service in Inverclyde. She spearheaded the development of a dedicated ‘transition’ clinic for older adolescents after identifying a gap in care for this group. Previously, those aged 17 or over who were waiting for assessment and/or treatment were frequently transition to adult services when they turned 18. The new clinic provides immediate access, assessment and treatment for young people aged 17 years and 6 months and older.
This initiative has provided timely access to care and treatment for mental health concerns, and has facilitated further assessments and exploration of diagnoses such as autism spectrum disorder and attention deficit hyperactivity disorder, as well as cognitive difficulties. The results have been overwhelmingly positive, including improved mental health outcomes for young people, prevention of deterioration, timely neurodevelopmental diagnoses and treatment, and a reduction in referrals to adult mental health services.
Hannah Grant, Advanced Practice Dietetic Led Coeliac Service NHSGGC
Hannah has successfully transitioned the Coeliac Disease service from a consultant-led to a Dietetic Led Coeliac Service, marking a significant advancement in patient care. This initiative addresses the lifelong management of Coeliac Disease, which requires the strict elimination of gluten from the diet. Over the past two years, Hannah has implemented a streamlined process ensuring timely access to diagnosis and dietary interventions for all patients, significantly reducing over 300 unnecessary biopsies.
The service prioritises patient-centred care by allowing dietitians to manage all referrals from primary and secondary care, ensuring that medical colleagues can focus on the most critical cases. This innovative model not only enhances patient care but also optimises resource utilisation within the healthcare system.
What makes this service truly special is its status as the first dietitian-led clinical pathway in adult gastroenterology at scale. Hannah’s evidence-based approach has revolutionised the treatment of Coeliac Disease, demonstrating the essential role of dietitians in gastrointestinal management and improving patient outcomes through dietary changes.
QEUH Fetal-Genetics Group
The aim of the Fetal-Genetics Group team at the Queen Elizabeth University Hospital was to change the clinical experience for patients and families planning or undergoing a pregnancy where there is a known family history of a genetic condition and/or pregnancy loss. When a routine ultrasound scan shows some fetal anomalies that may be due to a genetic cause, this can result in a period of worry and distress for the patient/couple until more information is available, so time is of the essence to either reassure the patient/couple or equip them with the appropriate information to help them make informed choices about their pregnancy and/or postnatal care.
The Fetal-Genetics Group combines the skills of Consultant Obstetricians, Specialist Midwives, Consultant Geneticists, Genetic Counsellors and Clinical Scientists to provide a truly multi-disciplinary approach that allows the most appropriate support and information and any genetic testing to be made available to this group of patients at the earliest opportunity and throughout their pregnancy and beyond.
Scottish Epilepsy Register
The Scottish Epilepsy Register has been developed under the leadership of NHSGGC Consultant Neurologist Dr Craig Heath and Johnathan Todd, Head of Information Management. Epilepsy is one of the most common neurological conditions, with an estimated 55,000 people living with it in Scotland. The Scottish Epilepsy Register uses routine health data, collected via a clinical dashboard, to provide an alert to healthcare professionals following a key adverse event. Its main aim is to reduce excessive mortality and morbidity in epilepsy and to improve access to care and outcomes in people living with the condition.
As part of the project, key pieces of clinical information are collected from other health boards which will be used to create a Scottish National Audit Programme for Epilepsy, allowing trends and outcomes to be tracked and monitored. Once fully established, the methodology could be applied to other chronic neurological diseases to improve disease recognition and management.
Better Health
This award commends staff who have implemented an initiative to improve the health and wellbeing of patients, the public and/or staff.
Nominees
Pain Management Service
The Pain Management Service has recognised for a long time, significant health inequalities and barriers to access for patients with communication support needs. For non-English-speaking patients, language barriers often create significant challenges when navigating the healthcare system. This is particularly true in specialised services like pain management, where understanding treatment options and communication with healthcare providers is critical for successful outcomes.
The service made it their priority to break down these barriers and improve accessibility, ensuring that every patient has the support they need, in the language they understand. To help achieve this and informed by patient and staff feedback, the team launched a number of initiatives from revision of patient materials to incorporating pain management into interpreter training.
The result has been a whole system approach bringing better accessibility for patients for whom English is not their first language and greater engagement with healthcare services, and as well as enhancing the patient experience the initiative has also strengthened the clinical team.
Gillian Harvey, Health Improvement Lead (Acute)
Gillian has been instrumental in addressing health inequalities through her leadership of the Support and Information Services (SIS) team at NHSGGC hospitals. She spearheaded crucial initiatives like the Emergency Food on Discharge program, ensuring that no patient leaves the hospital without food. These programs are now core services, sustained despite budget constraints.
Gillian also developed the Home Energy Crisis Response Service, which helps patients safely return to warm homes—a vital component in preventing delayed discharges. Her team actively engages with vulnerable populations, offering financial advice and support to those facing poverty. In 2023-24, SIS facilitated 3,762 referrals to financial inclusion services, resulting in over £4.5 million in financial gains for patients.
Gillian’s exceptional leadership has fostered a motivated SIS team that provides holistic support, ensuring that patients receive the assistance they need while navigating the challenges of the cost of living. Her commitment to tackling health inequalities is both impactful and inspiring, making her a deserving nominee for this award.
The Apple Clinic: prehab into rehab – Clyde
The Apple Clinic is a multidisciplinary team covering the Clyde sector, with the shared aim of getting patients in the best physical and mental health before, during and after their surgery. The team provides prehabilitation-into-rehabilitation and have been running the clinic for nearly 10 years and have seen between 500-600 patients. They assess each surgical patient and refer them for exercise and physical activity at either their own exercise classes, or to community partners, local charities or private services.
Physiotherapists Mhairi and Louise Crookston run the Inverclyde Royal Hospital Apple Clinic. They run weekly group circuit classes for patients awaiting surgery, which family members can join to provide support. The clinic has been transforming the surgical department by engaging nurses and Allied Health Professionals trained in exercise, health advice and cognitive behavioural therapy, all of which has reduced complications, shortened hospital stays and improved post-surgical recovery for patients.
Better Value
This award is for staff who have increased efficiencies taking a new approach to work making better use of resources.
Nominees
North West Primary Care – Zendesk
Zendesk aimed to streamline community pharmacy queries to enhance patient care in the North West of Glasgow City. Utilising the platform, community pharmacies submitted queries online rather than by phone, allowing for quicker and more efficient handling. Key objectives included routing queries to appropriate pharmacy team members, reducing administrative workload in GP practices, and improving turnaround time for medication-related issues.
Launched in November 2024, the system handled 435 queries in two months, with 81% resolved by Pharmacy Support Workers, thereby freeing up over 60 hours of pharmacist capacity for face-to-face patient care. The initiative not only saved staffing costs—almost £850 in eight weeks—but also provided self-help resources for community pharmacies.
With expectations to handle over 15,000 queries annually, the project is set to release nearly 2,100 hours of pharmacist time and achieve annual savings of approximately £31,000. This innovative use of IT to direct workload enhances service efficiency and patient safety.
NHSGGC Biorepository
NHS Greater Glasgow and Clyde’s Biorepository is the first in the UK to achieve accreditation to ISO20387:2018, the new biobanking standard. It was awarded this by the United Kingdom Accreditation Service (UKAS), the UK’s national accreditation body, becoming only the eight biobank in the world to achieve this. There have been many improvements to the Biorepository’s quality processes and this has improved the service it provides to academic and commercial researchers, supporting their world leading medical research with access to surplus diagnosis tissue and blood.
Accreditation against an ISO standard is a key indicator of high-quality processes and technical competence in the handling and storage of tissues used for research activities.
The Biorepository, based on the Queen Elizabeth University Hospital campus, stores and provides access to a wide range of human tissue for use in valuable medical research into a range of diseases.
Dry Mouth/Sjogrens Multi-disciplinary clinic at Glasgow Dental Hospital
The clinic was set up in 2024 to provide a one-stop service for patients with symptoms of Sjogrens disease. Sjogrens is an autoimmune disorder with an increased lifetime risk of lymphoma development, and its diagnosis involves a range of investigations previously undertaken over three appointments.
By establishing the clinic – the first of its kind in Scotland – Consultants in Oral Medicine and Dental Radiology have enabled all the necessary investigations to be undertaken in a single appointment, allowing patients with negative results to be discharged to their general dental practitioner after one visit and patients with confirmed Sjogrens to have their cases managed more efficiently.
In the first six months of operation, this new approach saw 30% of patients seen by the clinic discharged after their initial visit, saving around 60 future appointments with Dental Radiology and Oral Medicine. The effect of patient experience has been positive too, and in local questionnaires, every patient has appreciated this more streamlined approach.
Better Workplace
This award recognises the often unseen work of our staff who help make NHSGGC a better workplace, improving the culture and supporting colleagues.
Nominees
GGC Allied Health Professions Practice Education Team
The GGC Allied Health Professions (AHP) Practice Education Team aimed to enhance the educational experience for students and AHP staff within NHSGGC by implementing a multi-dimensional education programme. The AHP Director prioritises an inclusive education strategic framework for 12 healthcare professions, including AHP Health Care Support Workers (HCSW), ensuring access to innovative learning opportunities for the current and future workforce.
The Practice Education Team has played a pivotal role over the past two years by collaborating with key partners, improving communication, and designing new AHP educational opportunities. Their efforts have raised the profile of AHPs, transformed NHSGGC’s educational offerings, and supported career development for staff and students.
Key deliverables include enhancing practice-based learning placements, developing a funded modular programme in collaboration with Glasgow Caledonian University, and supporting HCSW workforce development through flexible programmes. The team also plays a vital role in staff support during the recovery renewal period, leading initiatives like the Return to Practice programme and promoting clinical skills through simulation.
Their commitment to education governance and service improvement significantly contributes to the overall wellbeing and professional growth within NHSGGC.
Internationally Educated Nurses Oversight Group
The Internationally Educated Nurses Oversight Group aimed to enhance recruitment, professional governance, and pastoral care for Internationally Educated Nurses (IENs) joining NHSGGC. By facilitating discussions among multi-disciplinary professionals, the group streamlined support for IENs addressing key concerns like visa processes, accommodation, and education. Members included Human Resources, Senior Nursing Managers, and Practice Education, ensuring collaborative efforts to foster a positive working environment and address IENs’ needs.
The group’s success is reflected in several impactful initiatives: the creation of a welcoming NHSGGC handbook, improved collaboration with Higher Education Institutions for upskilling, regular staff presentations to address IEN challenges, and the introduction of a ‘My Nurses Life’ workbook. Additionally, a dedicated website for IENs was launched, alongside the first-ever ‘Welcome to the UK Workforce’ workshops held in Scotland.
In 2023-24, NHSGGC became the leading board in Scotland for employing IENs, successfully adapting strategies based on feedback from the previous cohort. This comprehensive approach not only enhanced integration but also cultivated a culturally aware and psychologically safe environment for IENs.
Stacey Kavanagh – Nurse Team Lead, South alcohol and drug delivery service in Pollok
Stacey is a manager who has created a workplace that is not only comfortable but also supportive and inclusive for everyone. She consistently looks out for her colleagues, offering guidance, encouragement, and a listening ear, and has created a team where everyone feels valued.
She ensures that all work progresses smoothly, addressing challenges proactively and stepping in to help when difficulties arise, while she actively encourages and supports team members in their professional growth, providing mentorship and opportunities to learn and advance.
This approach has fostered a positive, inclusive and efficient work environment and ensures her team feels supported, motivated, and well-equipped to handle both day-to-day tasks and challenging situations.
As a result, the team has seen improved efficiency and productivity, while there has been a noticeable improvement in staff retention. Numerous team members have expressed their appreciation for Stacey’s leadership, approachability, support and commitment to fairness, and have noted an increase in job satisfaction as a result.
Nursing and Midwifery Council (NMC) Referrals Database (Rob)
The aim of the project was to redesign the NHSGGC database and governance process for NMC referrals, enhancing data protection and confidentiality while improving communication channels. Identifying risks in the previous system, Michelle Murray-Moore undertook training to explore innovative IT solutions that would streamline information sharing within the NMC referral process. Collaborating with Tracy Donaldson, they developed a user-friendly database with effective reporting functionalities and key document templates.
The success of the new system has been recognised by senior nursing and midwifery managers and the NMC Regulatory Adviser, highlighting several benefits: a robust governance process, a clear single point of contact, user-friendliness, and flexibility for future adaptations.
This initiative has remarkably improved NMC referral management, fostering transparency and maintaining confidentiality for staff under investigation. It has significantly enhanced efficiency, enabling the NHSGGC team to respond promptly to NMC and service colleague requests and freeing up resources for other important workstreams within the Directorate. This impactful achievement exemplifies innovation and dedication to excellence in healthcare governance.
Global Citizenship
This award recognises staff who have travelled overseas to provide healthcare and/or education in developing countries or countries in crisis.
Nominees
Breast cancer care in Gaza
Breast Cancer Advanced Nurse Practitioner Gerry O’Hare and Dr Abdulla Alhasso, a Consultant Clinical Oncologist, bring a combined 20 years of experience in supporting cancer care in Palestine, with a particular focus on breast cancer in Gaza. Breast cancer outcomes for women in Gaza are significantly worse when compared to neighbouring countries and international benchmarks. Gerry and Abdulla have undertaken regular visits to Gaza over the past five years, which has been done in their own time and with the support of the Medical Aid for Palestinian organisation.
They collaborate with healthcare professionals in Gaza to enhance the clinical outcomes for women diagnosed with breast cancer by improving both their diagnosis and treatments. The pair also participate in weekly online multidisciplinary meetings with Palestinian colleagues to discuss optimal care for women presenting with early and advanced breast cancer, while also navigating the extremely challenging local circumstances.
Professor Sameer Zuberi – Paediatric Neurosciences Unit, Royal Hospital for Children
Professor Zuberi is a committed advocate for epilepsy care in children across at a national, European and global level. He is an active participant in international research, and his work has helped in improving the diagnosis, treatment and care of children with epilepsy, improving their quality of life and allowing them to achieve their potential in life, education and future career.
He makes regular use of vCreate, a technology by which parents send video clips to clinicians who can advise, in real time, on the significance of an event that worries parents and also helping make a diagnosis in difficult cases of epilepsy
He has chaired the European Paediatric Neurology Association and played an important role in the twinning of the Royal Hospital for Children with the Children’s Hospital in Karachi, Pakistan. He had helped to foster links with and training and support for neurologists in Ukraine as well as supporting efforts to train and educate colleagues working in Palestine and Gaza.
Dr Mark McAuley GP Partner Regent Gardens Medical Practice Kirkintilloch, Assistant Director of General Practice for West of Scotland (NHS Education Scotland)
Dr McAuley, a partner at Regent Gardens Medical Practice for over 25 years, and Assistant Director of General Practice for West of Scotland (NHS Education Scotland), has demonstrated exceptional commitment to both his local community and global health initiatives.
He has volunteered with Freedom from Torture for over 11 years, where he provides medicolegal assessments for survivors of torture, ensuring their human rights are upheld through rehabilitation support. His extensive training allows him to document the physical and psychological effects of torture, aiding asylum seekers and refugees in rebuilding their lives.
In addition, he has contributed to the development of primary care in India through his ongoing partnership with CMC Vellore. He conducted a successful training workshop in October 2022, which spurred further engagement and recognition at international conferences. As a PRIME tutor, he has also visited Albania multiple times to enhance family medicine training.
His selfless dedication to these global initiatives while providing exemplary care to his local patients makes him a deserving nominee.
Nursing and Midwifery
This award recognises nurse(s) who demonstrate the best qualities of patient care and the ethos of nursing.
Nominees
Brachytherapy Nursing Team
Nurses on the Beatson’s B3 ward are a highly specialised team helping to care for women with gynaecological cancers. They deliver brachytherapy, a type of radiotherapy that gives radiation inside the body and run the only nurse-led service in Scotland for women who require this treatment. The nurses pre-assess and examine patients and insert the necessary cylinders to allow patients to receive high dose radiation within a specialised unit.
This is a regional service for patients attending for sealed and unsealed sources of treatment. Melanie Whyte, Senior Charge Nurse, has been instrumental in helping to develop and implement the necessary protocols, safety advice and training for nurses in the unit. Patient feedback has confirmed patients attending the unit are happy with the service, and turnaround time has improved service delivery while also taking a huge time commitment away from Senior Consultants who previously carried out these treatments.
Susan Hunt, Professional Nurse Lead GPN/ANP
Susan was closely involved in efforts to enhance excellence in care within NHSGGC by supporting trainee Advanced Nurse Practitioners (ANPs) in developing the knowledge, skills and competencies required for advanced practice. In collaboration with NHSGGC Advanced Practice corporate team and Glasgow Caledonian University (GCU), she developed and delivered a hugely successful work-based Masters-level learning module to support trainee ANPs to reach the level of extended practice expected of them.
The module is facilitated by Susan and trainees are given a safe space to discuss individual clinical cases which allows for open discussion and joint learning, as well as facilitating peer support and engagement. Her ability to engage trainees on a personal level helped the trainees navigate the complexities of their new roles, providing reassurance and guidance, and ensuring they felt valued and supported.
Around 120 staff have competed this module and have gone onto work as ANPs. The result is a stronger, more skilled ANP workforce, improving patient care and making a lasting difference in primary and community healthcare services.
Tissue Viability Team (Dykebar)
The Tissue Viability Nursing Team at NHSGGC, a cohesive group of 10 nurses, is dedicated to supporting patients with complex wounds, receiving up to 850 referrals monthly. Renowned for their expertise, this team implements innovative, person-centred initiatives that enhance care while effectively using resources.
One key initiative focused on reducing unnecessary documentation, which previously consumed up to three hours per shift. They developed an ABCD system that emphaises meaningful record-keeping and effective communication. Additionally, they transformed patient repositioning practices by moving away from ritualistic two-hour checks, allowing for more personalised care that improves patient comfort and nursing efficiency. This approach, supported by evidence from case reviews and focus groups, has led to significant time savings and better patient outcomes.
The team enhances education through engaging workshops, utilising games such as wound care bingo and interactive quizzes to facilitate learning. Their efforts have gained international recognition, influencing wound care practices across the UK and beyond, and have been published in peer-reviewed journals, showcasing their commitment to advancing wound care.
Volunteer
Recognising people who go the extra mile contributing tirelessly and providing outstanding help and support for the benefit of others.
Nominees
Morag Brierton, RAH volunteer
Morag is NHS Greater Glasgow and Clyde’s longest serving volunteer in acute services, having volunteered with the organisation for over 15 years. She is a Volunteer Driver for the Royal Alexandra Hospital Health at Heart team and transports patients to and from the hospital for cardiac rehab exercise classes in the Health at Heart gym. Within the service, patients also receive physiotherapy, education sessions, practical advice and emotional support, helping to rebuild their confidence and come to terms with a range of different heart conditions.
Transport within and around Renfrewshire to the hospital can be challenging, particularly for patients living in semi-rural areas. But Morag’s vital support helps break down barriers for patients – many of whom are older and at risk of isolation – in accessing the rehab programme. They enjoy spending time with Morag in the car having a chat, and she builds strong relationships with them over the weeks she is picking them up and taking them home.
The Growing Spaces Garden Volunteers – Gartnavel
The value of greenspace to our health and wellbeing is well documented, and the Garden Volunteer team are central to NHSGGC’s efforts to offer multi-purpose spaces in nature, where patients, staff and the general public can find a place to relax, meet friends or simply have a moment of peace.
The volunteers work throughout the year to maintain the garden spaces at Gartnavel, and thanks to their skills and foresight, they have developed a donation stall on which are offered plants for visitors and participants who use the gardens. This helps sustain the current infrastructure as the garden has no allocated budget. Surplus produce and cut flowers are shared with patients and staff throughout the campus.
They are the welcoming face of our Growing Spaces and work with a range of third sector organisations, as well as staff and patient groups, to share and promote the benefits of our greenspaces. They are always looking to improve their work and will happily act on suggestions, attracting positive feedback from those who visit the gardens.
Queen Elizabeth University Hospital – Volunteer Welcome Guides (10-year anniversary)
When the Queen Elizabeth University Hospital opened to the public in spring 2015, a team of 100 volunteers were recruited to be the friendly faces people needed when arriving at one of the largest acute hospital campuses in Europe. Ten years later, 30 of those 100 people are still actively serving as welcome guides, marking a decade of commitment.
The volunteers come from a diverse range of backgrounds and include former patients, NHS employees and aspiring medical students, as well as a 91-year-old participant which is truly inspiring. This long-term dedication and diverse experience undoubtedly contribute significantly to the welcoming and supportive atmosphere.
The welcome guides play a vital role in supporting patients, families and visitors and helping to alleviate stress. By dedicating on average 150 hours per week, they ensure a positive experience for those entering the hospital and help to guide individuals to their desired destinations.
Was this helpful?
Yes
No
Thanks for your feedback!
The local staff awards are popular across all Directorates and HSCPs as they enable all areas to recognise and show appreciation to colleagues who have gone the extra mile. Everyone can give their own examples where amazing care or services have been delivered under hugely challenging conditions and staff have nominated the colleagues who they think most deserve recognition for their stand-out efforts, skills and commitment.
Presentations have been held in each local Directorate and HSCP to award the winners in categories including Employee of the Year, Team of the Year, Leader of the Year, Innovation of the Year and Volunteer of the Year, with the overall winner announced at the Celebrating Success Staff Awards Event on 28 May 2025.
You can find out more about each of the overall winners in each category below, read about the nominees who were shortlisted, and you can also view photos and videos.
The winners were announced live on the night on our social media channels (follow the #ggcawards tag).
Congratulations to all our winners and nominees!
Acute Services – Clyde Sector
Overall Winner Nominees
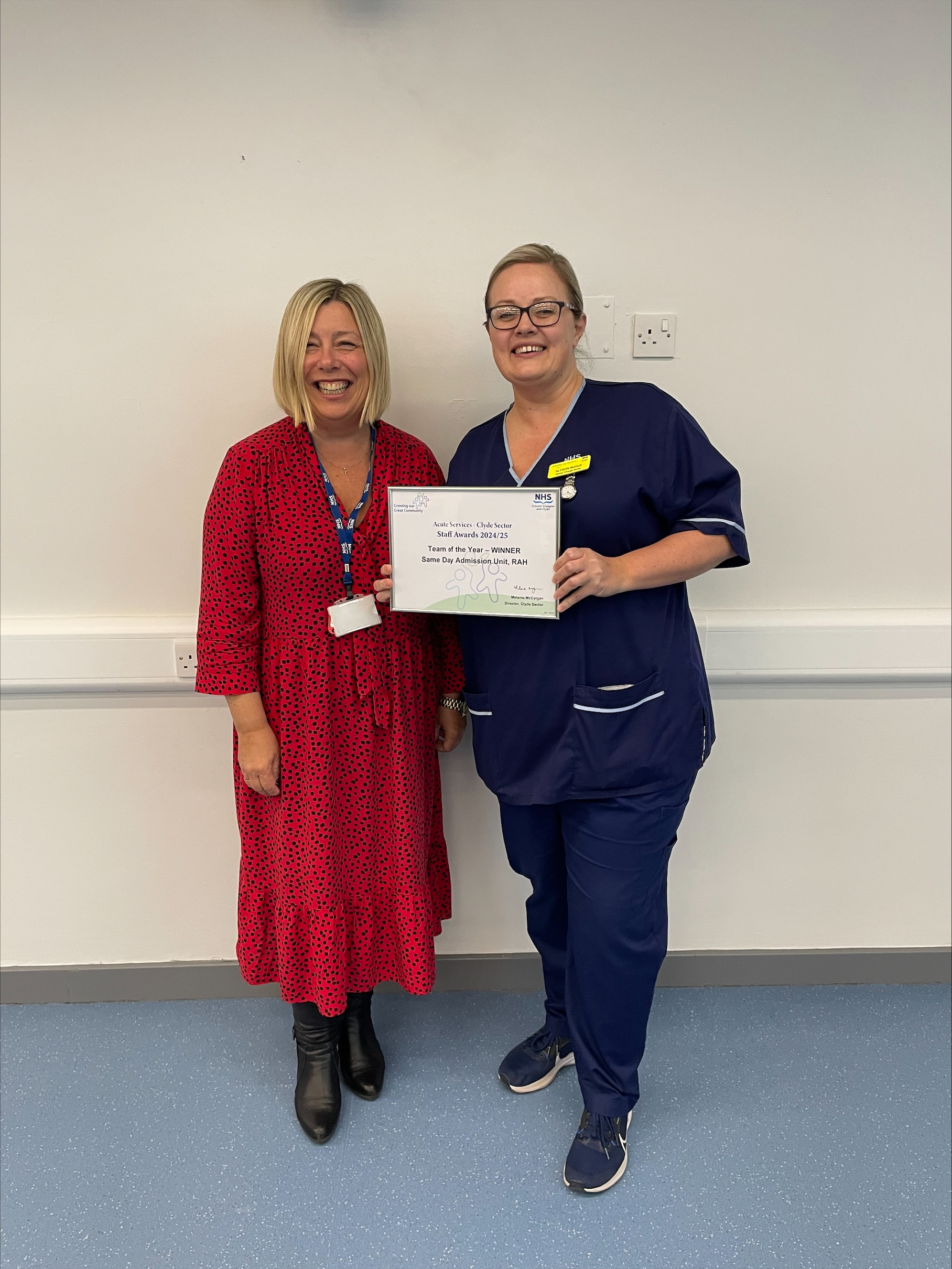
Team of the Year
Same Day Admission Unit (SDAU) RAH
The SDAU team works collaboratively to ensure patients are at the forefront of everything they do, deliver the best care, avoid delays for theatres, and provide support to other services.
SDAU is a Monday to Friday elective surgery unit, comprising 14 trolleys and 2 chair establishment. At present the unit is open 24 hours per day, 7 days per week due to bed challenges on-site.
The team’s responsiveness was evident when the unit accommodated eight patients each night throughout January, supporting the hospital by easing pressure on wards to allow flow, and enabling surgeries to continue despite service challenges.
Megan has been a huge support for the Older People and Stroke Services team, working closely with the Clinical Service Managers and Lead Nurses to assist the directorate. She has a fantastic understanding of the services and proactively queries aspects with the team.
Megan has supported new team members in learning how to manage budgets and analyse reports, and this has contributed significantly to building financial knowledge and confidence within the team.
Leader of the Year
Dr Gautam Ray, Consultant Physician, Acute Medicine, RAH
Gautam was instrumental in setting up the Quality Improvement Den at the RAH in 2018. This opportunity has now been expanded to support colleagues across the Clyde sector.
The Den provides assistance and guidance for colleagues to pursue QI projects across a wide range of services, resulting in a skilled workforce and valuable improvements to patient care.
Cohort 7 is now underway, and over the years since the Den commenced, in excess of 127 colleagues have participated in it, delivering a broad range of improvement projects and encouraging a culture of continuous improvement across Clyde sector.
Innovation of the Year
The Apple Clinic : Pre-habilitation & Rehabilitation for cancer and surgical patients (Mhairi Burke & Elaine Crookston, Physio, IRH)
The Service was expanded to IRH in Dec 2023, enabling a sector-wide approach for Pre-habilitation. During the past year, this has extended to include a Rehabilitation phase post-surgery and during other cancer treatments. In addition, a pilot model was introduced to educate family members how to support their loved ones
The Clinic is a sustainable model, embedding research, and engaging nursing and AHPs trained in exercise, health advice, cognitive behavioural therapy. This approach has reduced complications, shortened hospital stays, improved post-surgical recovery. The initial clinic has supported 50-60 IRH patients and families. IRH is the only site now consistently delivering prehab/rehab in West of Scotland Cancer Network.
Volunteer of the Year
David Roy, AHP Rehab Support Volunteer & Rainbow Garden Volunteer, IRH
David’s primary role is as a Rehabilitation Support Volunteer, working on a weekly basis on the Stroke ward at the IRH Larkfield Unit.
He works alongside the AHP team, supporting patients to enhance their mobility and recovery. In addition, David provides companionship and support, to help promote patient’s mental health and well-being.
David is also a volunteer member of the Rainbow Garden, where he helps keep this valuable therapeutic outdoor space clean & tidy alongside his fellow volunteers.
The unwavering support and encouragement David provides in both his roles is hugely appreciated by patients and colleagues alike.
Acute Services – North Sector
Overall Winner Nominees
Team of the Year
North Frailty Team
The North Frailty Team is a multidisciplinary group dedicated to improving care for older adults with frailty. Working alongside ED and AAU, they streamline patients to a specialist unit for timely Comprehensive Geriatric Assessments (CGA). Their innovative pathway has reduced the median length of stay from 16 to 11 days without increasing readmission rates. They introduced a CGA Huddle, integrating community teams to support early discharge.
Their commitment to person-centered care, collaboration, and overcoming resistance to change has enhanced hospital flow and patient outcomes. Patient feedback highlights their compassionate and high-quality approach, demonstrating that getting care right for older adults benefits everyone. Their dedication and teamwork make them truly deserving of this award.
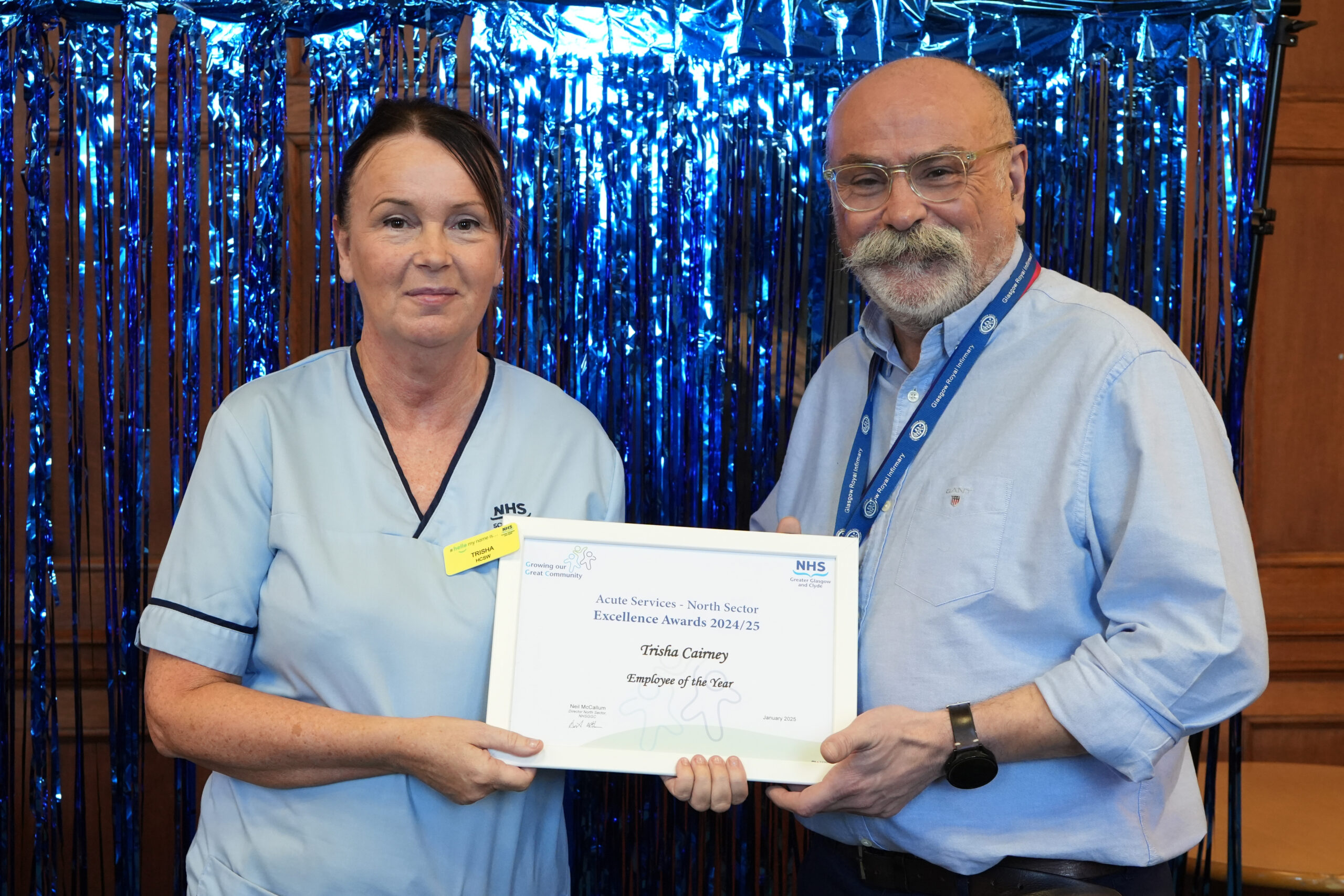
Employee of the Year
Trisha Cairney, Health Care Support Worker
Tricia, a Health Care Support Worker at Ward 43 (Cardiology), goes above and beyond in patient care and ward support. Despite the demands of a busy cardiology unit, she takes on additional responsibilities, including clinical audits, ordering resources, organising repairs, and infection control checks.
Her contributions have significantly improved ward performance in external audits. Tricia’s kindness and compassion make her a favourite among patients, bringing joy in their most difficult moments. A true team player, she supports colleagues selflessly and enhances the ward’s daily operations. Her dedication, quality, and teamwork embody NHSGGCs values, making her an outstanding role model and a truly deserving award winner.
Leader of the Year
Evelyn Taylor, Specialist Occupational Therapist
Evelyn has been a dedicated and integral member of the Occupational Therapy and AHP team at Glasgow Royal Infirmary for over a decade. A skilled practitioner and mentor, she supports staff development and has driven service improvements, particularly in Anxiety Management for COPD patients. Her work has reduced hospital admissions and facilitated complex discharges, empowering patients to manage their conditions.
Evelyn’s leadership, mentorship, and innovative approach have strengthened the OT service, earning her widespread respect. Her compassion, calmness, and unwavering support for colleagues make her a role model. Despite not holding a formal leadership role, her leadership influence is profound, shaping patient care and team development. Evelyn’s dedication, kindness, and professionalism make her a truly deserving award recipient.
Innovation of the Year
Elisabeth Waterhouse and Denise Carrigan – Practice Development Adult Acute Dietetics
The Dietetics team addressed recruitment challenges by redesigning the interview process to improve accessibility, inclusivity, and candidate experience. They introduced an online ‘meet and greet’ after work hours and provided support around interview questions, reducing candidate anxiety and improving response quality. Feedback from three interview cycles was overwhelmingly positive, with applicants feeling more supported and engaged.
Applications tripled, with a reserve list established to streamline future hiring. The initiative promotes dignity, respect, and neurodiversity while strengthening workforce planning. Recognised as best practice, this innovative approach has been shared across the AHP community, ensuring a more diverse, prepared, and sustainable workforce.
Volunteer of the Year
Lou Murphy, PA to the GM for Medical Specialties North Sector
Lou has been a key participant of the North Civility Saves Lives group, working to improve workplace relationships by promoting civil, caring, and compassionate interactions. She has facilitated focused awareness raising sessions across various departments, including meetings with consultants, junior doctors, and administrative teams. Her sessions encourage staff to reflect on their own behaviours and the impact of rudeness in the workplace.
Lou’s proactive efforts have been met with positive feedback, as she fosters discussions on promoting civility and reducing incivility. Her work exemplifies the values of dignity, respect, openness, and responsibility, contributing significantly to continuing to make the North, a NHSGGC a better place to work.
Acute Services – South Sector
Overall Winner Nominees
Team of the Year
Surgical Immediate Assessment Unit (IAU) , QEUH
The department is staffed by a combination of Healthcare Support Workers (HCSWs), Band 5 nurses, and Surgical Nurse Practitioners, with additional support from Advanced Nurse Practitioners (ANPs) and medical staff. This team works tirelessly to assess and implement the care needs of patients referred for surgical assessment by their GPs. They typically see a range of 730 to 750 patients per month and successfully discharge nearly half of them within four hours. Most discharges from the department occur between four and eight hours after arrival.
The team also runs Hot Clinics to ensure that patients do not remain in the hospital longer than necessary. If further tests are required, they arrange for patients to return for those procedures.
This exceptionally hardworking team deserves recognition for their contributions to unscheduled care.
Patient experience is significantly improved as most patients are seen within the four-hour target. Additionally, discharging patients to Hot Clinic slots reduces unnecessary waiting times for tests in an already busy department. This ensures that results can be discussed quickly after testing, allowing for effective further care planning.
The team is focused and driven, placing patients’ safety and well-being as their top priority.
Heather and Claire created an inhaler education station in the ward, which they updated monthly. They provided resources, quizzes, stickers, and QR codes for further learning. They collaborated with Respiratory Clinical Nurse Specialists (CNSs) and representatives to ensure they shared best practices and organised education days for the ward staff.
This initiative served as an excellent resource for the staff. In recent years, the variety of inhalers has increased significantly, and due to COVID-19 and staffing shortages, accessible education has been limited. Their educational resources offered a quick and convenient way to enhance staff knowledge. It was also shared with other respiratory wards and received a positive response.
Overall, this work improved patient care by enhancing staff understanding of inhalers, their functions, and proper inhaler techniques. This ultimately led to better administration for patients and increased understanding and usage, thus improving health outcomes.
Leader of the Year
Laura Campbell, SCN, Ward 8A, QEUH
Laura is a senior charge nurse on Ward 8A at QEUH, an acute care ward for older patients. She has demonstrated excellent leadership skills and a strong commitment to quality improvement within the ward, particularly regarding staff morale, infection control, and the overall standards of patient care.
After transferring from another area, Laura took the initiative to promote a more positive working environment, which led to improved audit scores and enhanced infection control standards. Her ability to enhance staff morale and motivation, as well as care and infection control standards, has been remarkable.
Laura’s dedication to the Older People’s Services Support team is evident each day and she has worked tirelessly to make significant improvements.
Innovation of the Year
Gill Reader, SCN, Acute Receiving Unit 5, QEUH
Gill led the development of the GGC: 322 Philips Cardiac Monitoring and Basic Rhythm Interpretation module, which is now a part of the LearnPro training platform.
This new module is designed to enhance staff training and education for caring for patients who require monitoring.
Gill also provided training in these essential skills, which will support staff in delivering quality care. The module is beneficial for staff development, allowing them to enhance their existing skills and learn new ones. It is now available organisation-wide on LearnPro, making it accessible to all staff. This resource is transferable to any department that requires ECG monitoring, representing a valuable opportunity for professional development and learning across all teams.
Diagnostics
Overall Winner Nominees
Employee of the Year
Jason Crooks, Operational Services Manager, Diagnostic Imaging
Jason, is an extremely hard working and experienced administration manager who took up his post of Operational Services Manager in December 2023.
Jason has over the last year made significant changes to ensure our performance monitoring and data is accurate. to support this he has developed a number of dashboards and systems to support the whole imaging team manage performance accurately. For example: Cancer tracking dashboard, Reporting discrepancy dashboard, a new share point site for imaging, Methods to meticulously manage Access and cancer funds.
Team of the Year
Radionuclide Dispensary
The Radionuclide Dispensary (RND) manufactures radiopharmaceutical medicines for Nuclear Medicine Departments across five Health Boards covering 60% of the Scottish patient population.
The current RND facility is isolated on the former Western Infirmary site. It has continued to operate through demolition of the WIG and the redevelopment of Glasgow University. The facility, while supported remotely, remains isolated.
The building has significant operational and logistical challenges and is unable to support necessary changes in technology and equipment.
The MHRA has a focus on the service, with bimonthly scrutiny.
There is an immense amount of pressure on the RND team to deliver a safe daily service to patients on a cancer pathway. For almost 10 years they have continued to manufacture and deliver radiopharmaceuticals to approximately 40,000 patients per year. In the most difficult of conditions, in the middle of a building site, managing a highly specialised service.
Regardless of the many challenges they have faced over this time, the team has delivered a safe patient service.
Leader of the Year (Joint Winners)
Andrew Reilly, Scientific Director
Andrew has integrated the clinical scientific service (DCPB) providing patient care for patients across the West of Scotland.
He has raised the profile of health care science both at local level and at National level.He advises the CMO as a Clinical Physics expert and is the IPEM Vice President Scotland, giving his energy to demonstrating the importance of health care science in patient care.
Despite being pulled in many directions Andrew always makes time for staff. He is welcoming and supportive, staff have direct access to him, giving freely of his time and wisdom in a kind and caring way.Focused and innovative, stimulating discussion opening the door to new ideas. He is very clear that no idea is a bad idea.
Over the last 18 months Andrew has supported the two areas where there has been no head of service – Radiotherapy Physics and Nuclear Medicine ensuring the clinical service was supported.He also lead the Radionuclide Dispensary and PET Production through pressurised MHRA and HSE inspections, supporting the whole way.
Andrew did all of this while recovering from an illness part way through the year. Many folk were not aware of this.His dedication and commitment to staff and patients is incredible always putting others first.
Nicola Wyllie, Senior Charge Nurse
Nicola is a patient focused Clinical Nurse Specialist who has been heavily involved with the Corporate Practice Development team and has developed educational videos on the care and maintenance of individual indwelling vascular devices these are now available on You Tube video to assist with the education and training of Nursing and medical staff across the NHSGGC health board.
In addition a competency framework is being developed for all staff who access specific vascular devices for administration of IV therapies. This competency framework will provide assurance that staff are appropriately skilled in the care and maintenance of vascular devices and ensure patients have the best care possible.
Innovation of the Year
Toxicology & Theraputic Drug Monitoring Service
Scottish drug-related deaths statistics show that drug misuse continues to be a significant problem. This has a direct impact on healthcare, including patients seeking help for drug use in primary care and hospital admissions across NHSGGC.
The Glasgow City Alcohol and Drug Partnership approached the QEUH Toxicology Team to discuss modernising drug screening; specifically, requesting an ability to detect a wider range of drugs.
As no commercial test kit was available to cover the range of drugs required, the Toxicology team developed a novel drug screen designed for local service users’ needs which was instrumental in the fight against drug-related deaths. Their innovation was a direct result of their ability to harness their collective brain power, knowledge, skills and experience to produce a transformative solution that benefited patients. The epitome of teamwork!
To date, over 14,000 patient samples have been screened using this test. A recent survey showed that service users agree that the extended screen they have developed has significantly improved patient management and had a positive impact on the population.
East Renfrewshire HSCP
Overall Winner Nominees
Team of the Year
Community Treatment and Care service
This nurse-led team deliver a range of services including ear care and wound care management.
The team are tasked to provide support GP Practices, and to help reduce treatment waiting times for patients.
As part of this they came up with an innovative new phlebotomy service, Bloods and Go.
The service operates in both Eastwood and Barrhead Health Centre and all 15 GPs in the authority can refer in. Since it launched in mid-June 2024, the service has taken bloods from over 10,000 patients and reduced waiting times for blood tests from days to just minutes!
Employee of the Year
Marion Evans
Marion is the one and only Business Support staff member for the very busy Community Mental Health Team.
She manages a varied workload in a fast-paced environment, looking after all business support needs for the service. Marion is exceptionally skilled and compassionate with service users, who often present in stress and distress.
Nothing is too much trouble for Marion, despite how busy she is. She is often approached by colleagues in other teams for help and she will always go above and beyond, without hesitation, to support them or offer advice.
Leader of the Year
Andrew Cuthbertson, Team Manager, Learning Disability Team
The LD team comprises a range of professions including social work, nursing, psychiatry, speech and language therapy, occupational therapy, physiotherapy, psychology and health care support workers.
Andrew has overall responsibility for the team, meaning he manages both Council and NHS staff, and this does require a specific skill set to ensure that the team works as one.
Andrew leads by example. His own passion, core values, calmness, positivity, integrity, work ethic and good humour are some of the attributes that make him an outstanding leader.
He is highly regarded and respected by colleagues, providers and the people we support.
Innovation of the Year
Fiona Gibson, Laura Herron and Amy Loveday
Occupational Therapist Fiona Gibson, Nurse Laura Herron and Assistant Practitioner Amy Loveday sit within the Older Person Mental Health Team and have been focused on stress and distress reduction in care homes.
Their integrated approach makes them the only team of its kind in GGC. Their innovative approach has:
Reduced the number of referrals and discharges within care home liaison service by 50%
Achieved a 50% reduction in the number of care residents with dementia on antipsychotic medication
Provided training to 101 care home staff
Prevented 14 care home placement breakdowns
Prevented 9 psychiatric admissions
Significantly reduced duty contact
Volunteer of the Year
Aileen Kane
Aileen has been fundraising for four decades. She starting with baking and selling cakes to her neighbours and over the years, her efforts have grown to include unique and joyful activities, such as walking with her family in tutus to raise funds.
She is also a walk leader, supporting people to get out and about. She has created a close-knit, supportive community and makes everyone feel welcome. For the past three years, she has organised a special Children in Need walk at Rouken Glen park, featuring memorable elements like a piper and a choir.
Going the Extra Mile
Mark Mulhern and Noleen McCormick
The duo won this award for continuously going the extra mile in their roles, displaying a positive can-do attitude and for regularly stepping outside their roles and responsibilities to support individuals, the health and social care workforce, and a wide range of partners across East Renfrewshire.
Mark is our Carers Lead and Noleen the HSCP Self Directed Support Implementation Manager and they have very busy day jobs.
Over the last 18 months, in addition to their substantive posts, Noleen and Mark have stepped up to support the Partnership with internal and external engagement, making a significant difference to our communities.
Wellbeing Champion
Claire Blair, Health Improvement Lead – Mental Health & Recovery
Claire is the ultimate champion for highlighting, advocating and supporting the health and wellbeing of the entire health and social care workforce.
Her kind, person-centred and empathetic personality helps bring people together. Claire has supported many colleagues through difficult times by being a listening ear, and sharing wisdom.
She also work in partnership with a number of organisations to support the delivery of wellbeing supports.
All of the judges were impressed by Claire’s ability to lead by example. She prioritises her own health and wellbeing, remaining resilient and positive, practices self-care, and makes use of wellbeing activities and resources.
Outstanding Contribution Award
Anne Marie Kennedy, MBE
At 86 years young, Anne Marie makes a substantial impact on people’s lives, volunteering a significant amount of her time, energy, knowledge and personality in supporting a wide range of individuals and services.
She shares her voice, opinion, and lived experience, alongside advocating for those who may not have the opportunity to do so.
She is the Chair of local charity, the wee red bus service, which transported 2145 residents to medical appointments in 2024 – that’s 4290 single journeys made by volunteer drivers.
Each year she organises a special volunteer celebration event and she is truly one of a kind.
Chief Officers Award
The Community Rehabilitation Service
The service demonstrates that fully integrated health and social care services create better outcomes for the people we support, and efficiencies.
This multidisciplinary team provide exceptional care, strive for excellence and are forward-thinking. They are also the only fully integrated service of its kind across NHSGGC.
Referrals have increased by 80% over the past six years and they have adapted to be able to manage this increased workload, and have modified their service to be able to meet the needs of our ageing population.
They’ve been central to the HSCP’s approach to reduce the number of avoidable hospital admissions.
eHealth
Overall Winner Nominees
Team Of The Year
eHealth and Clinical Teams involved in Ophthalmology Digital Patient Record
Commissioned by Scottish Government and in collaboration with clinical representatives from all Health Boards, eHealth National and Contractor Services, Information Management, Electronic Patient Record and Health Records teams worked together to develop and successfully implement the Ophthalmology Digital Patient Record and system.
This has been implemented across all NHSGGC Ophthalmology sites to connect primary and secondary eye care and enable transfer of patients between health boards. With the introduction of OpenEyes to NES Glaucoma Accredited Trained Community Optometrists, 749 patients have had their follow up care transferred to an Optometrist Practice near to their home.
Employee Of The Year
Alan Walker
Alan led and supported the testing and implementation of safer medicines projects including HEPMA and Pharmacy Stock Management (PSM). These are highly complex projects requiring extensive testing to ensure clinical and patient safety ahead of roll out. Alan has been commended for his approach and onsite support to clinical services through the implementations and embedding in business-as-usual practice.
Leader Of The Year
Lin Calderwood
Lin led key NHSGGC and national programmes of work including Ophthalmology Digital Patient Record and ANIA Digital Dermatology culminating in NHSGGC being the first Board to adopt both applications. Working with eHealth, clinical and wider ophthalmology service colleagues Lin led a positive and cohesive approach throughout.
Innovation Of The Year
eHealth Electronic Patient Record and Practice Development Nursing Teams
The collaborative effort of eHealth teams working closely with frontline staff to design and build patient centred nursing documentation tools within TrakCare. This project resulted in the completion of the nursing admission record, selection of risk assessments and a patient centred care plan. This reduces paper/scanning, supports audit activity and meets Healthcare Improvement Scotland (HIS) recommendations.
Estates and Facilities
Overall Winner Nominees
Team of the Year
Facilities Training Team
The Facilities Training Team has demonstrated exceptional dedication and teamwork, earning them the title of Team of the Year. This team has revolutionised the induction process for new facilities staff within GG&C by developing a comprehensive Corporate Facilities Induction Programme. Their innovative approach ensures that all new staff undergo a centralized three-day induction, covering essential policies, procedures, and mandatory training modules as well as delivering effective, practical training that will help them settle in their new roles. This program not only equips new employees with the necessary skills and knowledge but also provides a supportive environment for them to address any concerns before starting their roles as well as giving them a qualification they can use in future.
The team’s collaborative efforts have significantly improved the recruitment and onboarding process, ensuring consistency and high standards across the operational departments. Their commitment to enhancing the experience and skills of new employees has had a profound impact on the organisation. By working together and supporting each other, the Facilities Training Team has set a benchmark for excellence, making a lasting difference for both staff and patients.
Employee of the Year
Gerry Mather
Gerry Mather, a Project Manager within the Property & Capital Planning team, has been instrumental in ensuring the successful relocation of services from WGACH. He has been the primary contact for contractors refurbishing new locations, demonstrating excellent communication, negotiation, and persuasive skills. Gerry’s ability to maintain strong relationships with service leads and include all service and clinical requirements has been commendable.
Known for his calm demeanour and can-do attitude, Gerry is always ready to deliver a smile and tackle multiple tasks simultaneously. His dedication and positive approach have made him an invaluable asset to the department. As he retires at the end of March, this award would be a fitting tribute to his contributions. Gerry has also mentored junior project managers, sharing his wealth of experience and ensuring the continued success of the team. His efforts have significantly benefited patients and staff through improved facilities and service delivery.
Leader of the Year
Fiona Warnock-Greer
Fiona Warnock Greer, a Senior Project Manager within the Capital Planning team, has exemplified outstanding leadership through her management of the Parkhead Hub project, the largest primary care facility in the UK. Fiona’s dedication and teamwork have been instrumental in ensuring the project’s success, collaborating closely with diverse stakeholders, including HSCP, clinical areas, estates, facilities, design teams, contractors, and NHS Assure. Her leadership was particularly evident during the commissioning of the water system, where she established a short-life working group to ensure the highest standards were met. Fiona’s ability to navigate complex challenges, maintain clear communication, and foster a collaborative environment has been crucial in delivering a safe and functional facility.
Her proactive approach and commitment to excellence have earned her the respect and admiration of her colleagues. Fiona’s leadership has not only ensured the successful completion of the Parkhead Hub but also set a benchmark for future projects within the organisation.
Innovation of the Year
Brian Droy
Brian Droy, a CAD Operator within Operational Estates, has demonstrated exceptional innovation through his development of two critical pieces of equipment. Utilising his CAD skills, Brian designed an En-Suite emergency unlock tool for bathrooms and a transport cage for robots in the QEUH basement. These innovations have significantly supported both clinical and portering staff. The emergency unlock tool is particularly noteworthy, as it is being considered by other boards for its potential to provide immediate support to clinical colleagues during emergencies.
Brian’s proactive approach and ability to identify and address practical needs have made a substantial impact on operational efficiency and safety. His dedication to improving service delivery through innovative solutions exemplifies the spirit of the Innovation of the Year award. Brian’s contributions have not only enhanced the functionality of existing systems but also set a benchmark for future innovations within the organisation.
Finance
Overall Winner Nominees
Team of the Year – Joint Winners
Payroll Team
Working above capacity to sustain services while delivering key additional activities, including multiple retrospective pay awards, new pension regulations, increased pension applications, partial retirement provisions, system updates, and controls from the Reduced Working Week.
SSTS
Ensuring no impacts on SSTS service provision, including increased activity from Reduced Working Week updates, while integrating the new eRostering system to normal business. This includes supporting early adopters, initial rollout and support at the IRH site, piloting medics at QEUH ED, and supporting the HIS pilot of Safe Care for Adult Mental Health Inpatient areas.
Employee of the Year
Evelyn McIntyre
Evelyn has been extremely supportive to both the Management accounts team and the Sector management teams in a challenging year that has seen various changes in staffing as well pressures from gaps in sickness and vacancies.
Throughout the period of change Evelyn has maintained a professional approach and mentored junior staff members in their learning, advised management staff on a variety of issues, and maintained a high quality of service to key stakeholders. Evelyn continues help to shape the service of the management accounts function to meet the needs of the organisation.
Leader of the Year
Stuart McDade
Stuart has been pivotal in redesigning Ward Product Management (Stores) services at QEUH in 2023 onwards, focusing on ward layouts and stock cataloguing. Since April 2024, Stuart’s team completed stock reviews in 29 wards and improved the National Distribution Service (NDS) cage return process.
His leadership in training staff with new SOPs and training manuals has boosted team morale and performance. The Ward Product Management service at QEUH was recognised by the NSS Genesis team as one of the top 3 in Scotland.
Innovation of the Year
Joe Marr
Joe has shown exceptional dedication to his role at the Procurement Central Store (Dava St), particularly in 2024. He played a crucial role in the warehouse redesign, improving communication, simplifying processes, and enhancing governance by implementing signatures for goods over £1,000.
Joe’s efforts in updating the logistics schedule for QEUH have significantly improved the efficiency of inbound and outbound goods movement, providing clear guidance on delivery expectations. This project has freed up time for the Transport Team, allowing for better contingency planning and service readiness. Additionally, Joe has developed Procurement System SOPs for staff and consistently engages with management and other services to seek improvement ideas.
Glasgow City HSCP
Overall Winner Nominees
Team of the Year
Glasgow City HSCP Property Team
The Glasgow City HSCP Property Team has been recognised as Team of the Year for their outstanding delivery of the Parkhead Hub Project—the first project of its size and type within the HSCP. Despite competing demands, the team successfully engaged with Glasgow City Council, NHS Services, and key stakeholders to bring this vital facility to life.
Navigating challenges such as the NHS Assure process and a complex procurement landscape, they have worked tirelessly to ensure compliance and operational efficiency. Their dedication and teamwork have resulted in a transformational community space, including a library, café, and facilities for local groups, benefiting both HSCP services and the people of Glasgow.
Their commitment and resilience make them truly deserving of this award.
Employee of the Year
Liam Logue
Liam was nominated by his entire team for his consistent dedication and positive impact on his team. As a Social Care Worker for Housing First, Liam demonstrates a bright, supportive attitude, going above and beyond for both colleagues and service users.
Focussed on equality and high service standards, Liam has built trust with long-term homeless individuals, helping them navigate complex needs and engage with services. His personal kindness and proactive efforts, from sourcing clothing to providing gifts, make him an exceptional team member.
Liam’s commitment extends beyond his full-time role—he volunteers with a homelessness organisation, supporting the homeless and rough sleepers every Sunday. He actively encourages collaboration between the group and HSCP, bringing valuable insights to his work.
Leader of the Year
Pauline Ward
Pauline Ward has proven herself to be an exemplary leader within the Care Home Advanced Nurse Practitioner (ANP) Team, earning the Leader of the Year award for her exceptional leadership over just 18 months.
Pauline has redefined her team’s structure, raised care standards, and fostered a culture of collaboration. Her empathetic approach has maintained team morale during difficult times, demonstrating the true qualities of a leader who cares about the wellbeing of her colleagues.
Beyond immediate challenges, Pauline has cultivated a focus on continuous improvement, ensuring the team consistently exceeds care standards. Her leadership has had a lasting impact, improving communication, collaboration, and patient outcomes across the HSCP, solidifying the ANP Team’s reputation for excellence.
Innovation of the Year
The Thistle Project Team
The Thistle Project Team has been recognised with Innovation of the Year for its groundbreaking role delivering the UK’s first Safer Drug Consumption Facility. Led by Glasgow City HSCP, this project brought together a range of partners, including Glasgow City Council, City Building, NHSGGC, and several others, to create a service that addresses complex health and social challenges.
The Thistle is a unique service, the implementation of which required innovative solutions to many service requirements never previously encountered within UK health environments. Through extensive consultations with Lived Experience Reference Groups and the surrounding community, the team ensured the facility was tailored to meet the unique needs of users, with the potential to significantly reduce harm and influence future legislation.
Volunteer of the Year
Ross Parker and Paul Young
Paul and Ross have been recognised as Volunteer of the Year for their exceptional contributions at Gartnavel Royal Hospital.
Paul, a Garden Volunteer at the Growing Spaces, dedicates his time to maintaining the hospital gardens and supporting patients, staff, and visitors through gardening workshops and hands-on advice. His efforts help improve mental and physical wellbeing by creating a peaceful, nurturing space for all.
Ross, a Games Volunteer, provides a calming presence in the Hub Café, offering patients, staff, and visitors the opportunity to engage in games and meaningful conversations. His empathy and excellent listening skills contribute significantly to easing stress and anxiety.
Both volunteers have made invaluable contributions to the hospital environment, enriching the lives of those they support.
Human Resources & Organisational Development
Overall Winner Nominees
Team of the Year
Moving & Handling Team
The Moving and Handling Team provides support in complex patient moving and handling situations, providing safe and effective solutions for both the patient and for staff looking after them. Due to the pandemic and the need for a mass recruitment campaign, a significant backlog of staff in the nurse bank required training in Moving and Handling.
This training is needed to ensure compliance with national and local policy and is fundamental for safeguarding staff and patient safety.
Employee of the Year
Mark Allen, Senior HR Administrator, Staff Experience Team
Mark provides a fantastic administrative service to the Staff Governance Committee, Remuneration Committee and Workforce Equality Group.
Mark frequently supports other key initiatives within Staff Experience or across the broader HR Team, such as the EDI learning event or support for the Public Enquiry. In 2024, with the Head of HR Corporate leaving, Mark had to step in to lead much of the work around Remuneration Committee.
Leader of the Year
Gillian Gall, Head of HR, West Dunbartonshire HSCP
Gillian epitomises the values of the HR profession, very knowledgeable and works hard to learn and retain information so that she can provide timely and accurate advice and guidance. She is quick to recognise and praise achievements and encourages others to succeed. Gillian’s approach is having a positive impact on the perception of HR within the HSCP, and her influence extends to both WDC and NHS staff.
Innovation of the Year
Medical Bank Payroll, Craig Rennie, Workforce Planning & Information Manager
The Medical Bank Payroll has been manually handled for years since the Bank was commenced. This involved downloading all shifts from the Bank system and then typing them onto SSTS. This allowed payroll to pay the doctors.
Craig developed a solution that allows the process to be automated, reducing effort and increasing accuracy.
It has also been shared across the wider team, allowing for resilience around individual availability. The process has reduced from 4 days effort to 0.5 days effort.
Volunteer of the Year
Emma Kelly, HR Assistant, HR Support and Advice Unit
Emma introduced a weekly closed case report which pulls together information from various sources and presents it in a very user-friendly way. This clearly shows, week by week, how many cases have been closed, in what areas and for what reasons. It also has an interactive element which brings the report to life.
Emma also provides support to colleagues and develops database activity to support attendance management action planning.
Inverclyde HSCP
Overall Winner Nominees
Team of the Year
Children’s Residential Services (The View, Crosshill & Kylemore Children’s Houses)
The Children’s Residential Services Team in Inverclyde exist across three local houses The View, Kylemore & Crosshill who work around the clock to provide a loving and caring home for young people up to the age of 21. The team work extremely hard to provide a safe and nurturing home for children who are unable to reside with their families and they embody the core values of being child-centered, trauma-responsive and provide love and nurture ensuring that every child in our homes receives the support they need to thrive.
Beyond their crucial role in residential care, the team extends their reach to offer invaluable outreach services to families across Inverclyde, providing crucial support during evenings and weekends.
Employee of the Year
Laura Kenicer (Advanced Pharmacist, Primary Care)
Laura is an Advanced pharmacist within Inverclyde HSCP, she leads on Chronic Pain with the HSCP pharmacy team as well as being the professional secretary for the Scottish Pain Pharmacy Network. She has supported our pharmacy staff to deliver tier 3 opiate medication reviews, including training our staff on the administration, prescribing and patient counselling for naloxone. Furthermore, she supports the pharmacists develop clinically with her practice educator role.
Laura is passionate about supporting patients with chronic pain and those with issues with alcohol and drug misuse. She leads by example and is an inspiration to other staff.
Her passion for supporting these patients’ groups, encourages our team to take on advancing skills to also benefit the population of Inverclyde.
Gayle’s approach to recruitment ensured a team of dedicated individuals were introduced to the service to deliver support of varying intensities to meet the needs of each resident both in the Inverclyde Centre and in Temporary Furnished Flats in the community.
Gayle furnished a large communal lounge and a smaller lounge for outreach work, tirelessly engaged with third sector organisations and community assets to ensure residents received the care and attention of local dentists, opticians and student hairdressers who provided valuable services to make residents feel good about themselves.
She ensured they were trained in food hygiene to facilitate a brunch club three times a week providing wholesome and nutritious food to people who were hungry, and mentored residents in cooking and basic hygiene skills.
Innovation of the Year
Laura Gordon (Health Visiting Team Lead)
Laura had the idea of an App where parents and carers could access all the information that Health Visitors provide. Parents and carers will be able to access information that is safe and approved from their own mobile device at any time of night and day.
Links provided signpost to recommended guidance and supports and offer insights into children’s health, wellbeing, and development as well as a wealth of other relevant information. It provides reassurance for families, reduces the use of paper leaflets and ensures parents are not sourcing out of date or inaccurate information. The App is available to download now and will be officially launched this year. It is called Happy Healthy Tots.
Volunteer of the Year
Arlene Bissett
In addition to working and supporting her two adult sons, Arlene is involved in a number of local Inverclyde disability groups. Arlene’s close connections in the Inverclyde community makes her a source of information about voluntary organisations and things to do.
This helps other staff in the CLDT find out about activities people who use our service can access. Because her own sons are both active and contributing members of the community, she encourages others that people with neurological differences can be successful. She makes a difference to the young people who are members of the local Scouts, and to all the people who enjoy a meal from the Warm Kitchen.
Pharmacy Services
Overall Winner Nominees
Team of the Year
NHSGGC Primary Care Practice Educators
This programme, developed in 2023, was led by Tamara Cairney and delivered by dedicated Practice Educators across the HSCP teams. Over 2024, 53 pharmacists have been supported through the 12-week intensive period of supervision programme, beginning with a comprehensive Learning Needs Analysis.
This is aimed at developing pharmacists’ skills and confidence to manage increasingly complex patient care. This approach fosters the development of competence and autonomy, enhancing clinical decision-making capabilities. The program is designed to promote holistic professional growth by integrating reflective practice, patient feedback, and realistic clinical conversations. Pharmacists also have access to valuable well-being resources and are actively encouraged to collaborate within multidisciplinary teams, further enriching their learning experience.
Employee of the Year
Laura Kenicer Advanced Pharmacist (Primary Care)
Laura is an Advanced pharmacist who leads on Chronic Pain. She is a practice educator, supporting pharmacy staff to deliver tier 3 opiate medication reviews. This includes naloxone training on administration, prescribing and patient counselling.
She supports the HSCPs’ Alcohol and Drugs Partnership; chairs Inverclyde Drug Death Review Committee; co-chair of the Supporting Self-Management of Chronic Pain in Inverclyde Group; professional secretary for the Scottish Pain Pharmacy Network and is a member of the Inverclyde HSCP Mental Health, Alcohol and Drug Recovery and Homelessness Services Clinical and Care Governance Group. Laura is passionate about supporting patients and leads by example to inspire other staff, supporting them both professionally and personally. She is an amazing advocate for patients within Inverclyde
Leader of the Year
Susan Kafka Lead Clinical Pharmacist, Maternity Gynaecology and neonates
Susan demonstrates all the skills required to be a fantastic leader and role model.
She successfully implemented a planned re-design of Neonatal Pharmacy Service structure creating a peripatetic team for NHS GGC. Her engaging, inclusive style of leadership supported staff to engage with change, resulting in a smooth transition to the new structure.
This new flexibility has improved resilience and paved the way for standardisation and improvement of practices, supporting improved continuity of care for babies and their families. Under Susan’s leadership the team: demonstrate cohesive team working across 3 sectors; have shown great resilience through challenging times; support each other personally and professionally; are practising at their highest level and are involved in delivering service improvement or research.
Innovation of the Year
Pharmacy Technician COPD Patient Group Sessions: Improving Care & Developing the Clinical Role
Laura had the idea of an App where parents and carers could access all the information that Health Visitors provide. Parents and carers will be able to access information that is safe and approved from their own mobile device at any time of night and day.
Links provided signpost to recommended guidance and supports and offer insights into children’s health, wellbeing, and development as well as a wealth of other relevant information. It provides reassurance for families, reduces the use of paper leaflets and ensures parents are not sourcing out of date or inaccurate information. The App is available to download now and will be officially launched this year. It is called Happy Healthy Tots.
Director of Pharmacy Award
Hayley Miller and Sam Hayes
These individuals came together to act when they identified an opportunity to target waste and support the sustainability agenda.
They sent out information to staff detailing that medicines contribute to 25% of the NHS’s carbon emissions and invited interested parties to join a group so that everyone could all play a part in reducing our service’s carbon footprint. They encouraged change – big or small.
The new group, QECO, worked with a range of partners e.g. facilities, to establish site wide participation in change. Some initial changes included; implementation of site wide card recycling; reduced plastic bag use and an IVOST project in ICU. Future work is planned to maximise on national campaigns such as World Recycling Day in March.
Public Health
Overall Winner Nominees
Team of the Year
Public Health Protection Unit and Health Services Admin Team
The Health Protection and Health Services Admin support team is quiet, hardworking, modest, and kind, always doing their best to assist the Nursing and Consultant teams, even when overwhelmed. They are vital for supporting safe and knowledgeable practice, always smiling and maintaining a ‘can do’ attitude. An efficient support network is essential for clinical staff, especially during times of extra workload and pressure.
The PHPU Admin team is always present and their massive contribution is the backbone of the department, ensuring smooth functioning.
Employee of the Year
Louise Logue – Health Improvement Practitioner, Quit Your Way Smoking Cessation
Louise excels in providing smoking cessation support in NHSGGC’s Quit Your Way Community Service. She assists clients in West Dunbartonshire with intensive, person-centred support via phone and face-to-face clinics. Louise is dedicated, ensuring everyone receives 100% effort, and has built strong partnerships in the area.
Her exceptional support has garnered numerous positive patient stories on Care Opinion, praising her friendliness, knowledge, and dedication. Louise is also a supportive colleague, contributing to team improvements and assisting other Quit Your Way teams, such as the Pregnancy Service, during capacity challenges. Her commitment ensures the best service for all clients.
Leader of the Year
Susan Brodie-Adamson – Health Improvement Senior, Quit Your Way Smoking Cessation
Susan, the Team Lead for the Acute Quit Your Way Hospital Stop Smoking Service, is highly respected for her approachable, determined, and resilient nature. She is trusted to make the right decisions and is also known for her humorous and mischievous side, making her an ideal leader.
Susan encourages team members to shine, focusing on their strengths and helping improve weaknesses. She is empathetic, always ready to listen to work or personal issues, and quick to praise when deserved. Susan ensures no one struggles alone, always going the extra mile to support her team.
Innovation of the Year
Frontline Equalities Assessment Tool – Equalities and Human Rights Team
Over the past year, the Equality and Human Rights team implemented the Frontline Equality Assessment (FEA) tool across 40 wards and services. The Frontline Equalities Assessment tool assesses the integration of inequalities-sensitive practices, covering all protected characteristics. It evaluates patient data, communication support, and knowledge of related issues, policies, and discharge planning.
The tool includes a BME Pathway and an Autism Sensitised Pathway for further exploration. The tool helps staff reduce healthcare inequalities and identifies unmet needs, benefiting patients by removing access barriers. It ensures NHS GGC complies with Equality Legislation and the Public Sector Equality Duty, and informs the next Equality Scheme.
Volunteer of the Year
Brian Laidlaw – Support and Information Service (SIS)
Brian has demonstrated consistently his passion, commitment, and dedication to NHSGGC Hospital Support & Information Services (SIS) over the past 12 years. Recruited in April 2012, Brian has been a steadfast supporter of SIS frontline patient services, contributing weekly. His friendly, empathetic, and compassionate approach helps create a safe space for patients, carers, and families.
Brian balances the demands of healthcare volunteering with being a full-time carer for his wife. He is an integral part of the team, providing invaluable support to SIS workers and ensuring comprehensive care for patients and carers. NHSGGC SIS is proud to have him on their team.
Regional Services
Overall Winner Nominees
Team of the Year
Elder Ward Nursing Team, Rowanbank Clinic
The Elder Ward nursing team at Rowanbank Clinic were praised for the care shown to patients as they were awarded Team of the Year.
Colleagues who nominated the team highlighted their compassion and told how they were “consistently amazed at the strength and resilience shown” including the innovative and individualised ways they engage with patients.
Employee of the Year Regional Services – Alyson McArdle on behalf of Lorna Welsh
Lorna Welsh, an Advanced Clinical Nurse Specialist working in Haematology at the Queen Elizabeth University Hospital, was named Employee of the Year. She acts as a first point of contact for patients who’ve had bone marrow transplants and was praised for continually going “above and beyond” for those she cares for as well as her colleagues.
The service includes patients from across 12 Scottish health board areas, ranging in age and needs. Lorna’s expertise is often called upon from national and international organisations, including European Bone Marrow Transplant and the Anthony Nolan charity.
Leader of the Year
Lynsey Watt, Senior Charge Nurse, Ward B1, Beatson West of Scotland Cancer Centre
The Leader of the Year prize went to Lynsey Watt, Senior Charge Nurse in the Beatson’s B1 ward for Gynaecology and skin cancer patients.
She was described as having a “positive, can-do attitude”, with colleagues saying Lynsey’s dedication to person-centred care is significant and spans everyone she interacts with including patients, families and colleagues.
Lynsey was also praised for ensuring pop star Marti Pellow visited the ward to meet one of her patients, who couldn’t get out of bed, when he was at the Beatson recently to raise awareness of breast cancer symptoms.
Innovation of the Year
Magic Leap
This year’s Innovation prize went to staff at the Institute for Neurological Sciences who have been using a pioneering mixed reality (MR) system that allows them to “see inside” a patient’s body during surgery.
The MR goggles and system, known as the Magic Leap, are used by Consultant Neurosurgeon and Complex Spine Surgeon Mohamed Abdelsadg and colleagues to make surgeries less invasive and more accurate, minimising damage to other tissue.
The team were said to have “demonstrated remarkable dedication to advancing patient care by embracing cutting-edge technologies” that help to enhance precision.
Renfrewshire HSCP
Overall Winner Nominees
Team of the Year
Weavers Linn Team
Weavers Linn, a core part of our Learning Disabilities Service, is a dynamic and progressive service, known for their collaborative spirit and commitment to exceptional service user care. They proactively partner with other organisations to enhance support and ensure consistent, safe care and support. Their innovative approaches to service user progression are balanced by a professional yet fun atmosphere, creating a positive and supportive environment for both staff and service users.
Employee of the Year
Linda Murdoch – Public Affairs Manager
Linda is very motivated and hard working with an excellent customer focused attitude. She strives to ensure every complainant feels heard. Not only does Linda take time to talk to people and explain their options, but she listens and is able to genuinely help and offer good advice and comfort.
Leader of the Year
Ann Marie Cumming – Senior Business Support Assistant
Ann Marie has proven herself to be an outstanding leader, providing both guidance and unwavering support to her admin team and the wider district nursing team. Her leadership style is characterized by empathy, dedication, and an innate ability to inspire those around her. Ann Marie’s approach to leadership focuses on the wellbeing of her team, ensuring they feel valued, supported, and empowered in their roles.
Innovation of the Year
Well in Renfrewshire (WiRe) Map – Allan Mair and Carolyn Russell
The Well in Renfrewshire, or Wire, map displays information about the huge range of community groups and activities available across Renfrewshire in a visual and easy to use way. Our front-line workers as well as partner organisations and local people have been using it over the last few months to find out what’s available to them in their local area.
This is something that we have long been told is required. The map is evolving continually and Allan and Carolyn have been instrumental in liaising with partners in both the development of the technical side and in the gathering of the information.
Community Involvement Award
Thrive Under 5 Project
This programme takes a whole system, community food nurturing approach with the families of pre-school children, combining action on food and financial insecurity, healthy eating and physical activity. In the initial stages, the Health Improvement team led on the collection of data and information from partners around child health, poverty and food insecurity to allow comprehensive data analysis before constructing a community asset map model of two localities in Paisley Northwest & Johnstone.
Best Supporting Role
Change & Improvement Team
The Change and Improvement team is an invaluable part of the HSCP’s support services, working across operational services to make a significant and tangible difference to the quality of services the HSCP provides. The team plays a fundamental role in our successful delivery of policy, strategy, and our savings programme. Over the last year, the team has provided ongoing leadership and input to the Sustainable Futures programme, service improvement work and board wide activity.
As such the team’s contribution to progressing the strategic direction of the IJB and HSCP and supporting financial sustainability has been immeasurable and feedback has continuously noted the exceptional impact the team has had.
Chief Officer Award
CIRCLE Recovery Hub
Challenging times with restructures and reduced finances in Renfrewshire have seen a reduction in Support staff at CIRCLE Recovery Hub with the referral rates continuing to be high.
Our support staff have continued to give everything they have to support individuals in Renfrewshire that have mental health and / or addiction related issues, by continuing to develop the service provision, not only within one building but a Recovery Community in Renfrewshire as a whole. The integrity of partnership working and seeing their provision as a piece of a large support network has supported these challenging times and also built strong connections with partner agencies, which aligns to future goals of the RHSCP.
West Dunbartonshire HSCP
Overall Winner Nominees
Team of the Year
West Dunbartonshire HSCP Mental Health Officers
West Dunbartonshire HSCP Mental Health Officers collaborate with Medical and Legal professionals to fulfil the Statutory Duty to protect and support people experiencing mental health issues.
Every day, they go “above and beyond”, seeking to provide a person-centred, caring aspect to their work with those in the community who have reached a crisis point in their lives.
Forging strong relationships with their multi-disciplinary colleagues, they work closely together, offering peer mentoring and support which has significant benefits in terms of consistent and effective practice.
But their main focus is the people themselves – making sure they are fully included and engaged in their care as an equal partner whose voice is heard and then evidenced within their assessments.
As a key member of the West Dunbartonshire Alcohol and Drug Recovery Service, Gioia provides care, treatment and support to the most vulnerable people in the Community, making a difference every day.
Increasingly concerned at their lack of engagement with sexual health services, she completed additional training in this area of specialty, over and above her normal duties. Her qualifications have allowed her to commence a weekly Clinic which incorporates sexual health screening as well as other Harm Reduction interventions.
Collaborating with colleagues and services across West Dunbartonshire, Gioia is expanding this work further, promoting the benefits of regular healthcare, and delivering awareness training for service users to help them on their personal recovery journey.
A true inspiration to others!
Leader of the Year
Joyce Habo, Business Support Supervisor & PA to Chief Officer
Joyce provides valued support and guidance across West Dunbartonshire Health & Social Care Partnership.
Responding to current challenges, her leadership style has encouraged adaptability and resourcefulness to support the vision and direction of business priorities.
Mindful of the impact of change on her Team, she sought to create an environment fostering collaborative working and ongoing development, where colleagues still feel “cared for” themselves.
As a result, she has built credibility and earned the respect of her peers, the Senior Management Team and the wider organisation.
She fulfils an unconditional business support role with an attentive and efficient attitude towards everyone – showing empathy and a willingness to help, whilst being vigilant to the impact of an ever-evolving business landscape.
Innovation of the Year
MSK Project Team (Streamlined Vetting Process)
Reviewing and rebuilding the referral vetting process was a priority project for the MSK Physiotherapy service, ensuring patients receive the right care at the right time with the right clinician.
The MSK Project Team comprises a range of dedicated staff – from Health Care Support Workers to Advanced Practice Physiotherapy staff from MSK and Orthopaedics. Together, they met each challenge, completing project milestones within timescale.
As well as significantly improving patient experience, the new process makes more effective use of capacity for new appointments, maximising clinical skills and expertise at all levels.
Patient and Staff feedback has contributed to further improvements and the impact of the new process will continue to be evaluated as the project evolves.
Volunteer of the Year
Allison Graham, Low Back Pain Advanced Physiotherapy Practitioner
Allison has been described as “an exceptional Physiotherapist who is attuned to the diverse needs of the multi-cultural and socio-economic challenges of the patient population she serves.”
Her professional dedication is mirrored by her personal involvement in numerous initiatives aimed at fostering inclusivity and supporting under-represented groups.
One of these is the “Milk Enterprise Project” in Govanhill where Allison shows her commitment to empowering women from asylum-seeking and refugee backgrounds.
She volunteers her time to help them practice English and discuss health-related issues, providing vital support that extends beyond her day job, for example, establishing a weekly exercise class tailored to their needs, or organising a Quiz to help those preparing for the UK Residency test.
A very worthy winner!
Women & Children’s Services
Overall Winner Nominees
Team of the Year
RHC NICU
The Neonatal team at RHC has been outstanding during a particularly challenging time of displacement from the Neonatal unit. Despite having their intensive care unit flooded, necessitating a move to another area of the hospital, the team continued to
provide high-quality care to extremely sick and preterm babies. Their dedication and compassion have been remarkable, making them truly deserving of recognition for their incredible efforts and resilience. The team has pushed above and beyond all reserves to deliver high standards of care.
Patients in the neonatal unit can be very unwell, and a few of them will not make the journey to go home. The team is helping families to create lasting memories, treating everyone with dignity and respecting their individual needs and backgrounds.
Employee of the Year
Eleanor Quirke
Eleanor has been an exceptional employee and leader throughout her time in HPN, always demonstrating clear expectations delivered with care, kindness, and compassion. She listens actively and guides her colleagues through significant changes in maternity and neonatal services with unwavering optimism and hope. Eleanor’s trustworthiness, decisiveness, and willingness to take responsibility for her decisions have been invaluable.
She empowers her team, listens to differing views, and makes thoughtful decisions promptly. Her leadership has been integral to our success in neonatal service development, embodying the GGC values of respect and professionalism. Eleanor is a pillar of support and inspiration, making her truly deserving of this honour.
Leader of the Year
Mary Ross Davie
Mary has been awarded for her exceptional contributions as Director of Midwifery, driven by her compassionate and caring nature. Mary has transformed many aspects within the service. Her inspirational ways of working and unwavering commitment to high-quality service for all women and their families have been truly remarkable.
Mary unites the team with her positive vision, enthusiasm, and drive. Her care and compassion are evident in her work ethic and the care she demonstrates to both staff and women. Through her transformational work, she has fostered a positive culture within maternity services, emphasising dignity and respect. Mary’s approachable and empathetic nature allows her to bring staff along on her vision for change, creating a great team dynamic that ensures progress and continuous improvement of maternity services.
Innovation of the Year
Chris Hardwick
The same-day gynaecology operating initiative at New Victoria Hospital, led by Chris Hardwick with invaluable input from Claire Stewart and Vanessa Mackay, has revolutionized surgical opportunities for women on lengthy gynaecology waiting lists. By adapting existing pathways and guidelines and educating staff, they have significantly improved training opportunities for gynaecology trainees and nursing staff.
The day surgery team at New Victoria has harnessed their skills and knowledge to deliver highly productive theatre lists, resulting in shorter waiting times and positive postoperative experiences for patients. This innovative use of resources has not only enhanced staff morale and skill sets but also positively impacted other aspects of care and staff retention
Volunteer of the Year
John Lennox
John has been an invaluable volunteer at our respiratory clinic for many years, earning the respect and admiration of everyone in OPD RHC. He recognizes regular patients, ensures they check in correctly, and escorts them to other departments to keep things running smoothly. John’s contributions extend to the children’s charity, where he dons various outfits to make a better journey for our the patients. His respect, care, compassion, and empathy towards patients and families are evident in every interaction.
John is seen as an integral part of our team, keeping families, patients, and staff updated about clinic-related issues. His familiarity with the respiratory clinic’s operations and procedures used by doctors and multidisciplinary teams makes him truly deserving of the Volunteer of the Year award.
Rights of the Child Award
OPAT Team
The Paediatric Outpatient Parenteral Antibiotic Therapy (OPAT) service at RHC, established in December 2023, has been a beacon of excellence in providing safe and efficient care. This service allows children to receive intravenous antibiotics through daily hospital visits, rather than staying in the hospital, supporting their right to heal in the comfort of their home with family.
The OPAT service has significantly improved healthcare standards by developing new pathways, enhancing communication, and providing continuity of care. Between December 2023 and December 2024, 53 patients were managed by the OPAT service, saving 589 hospital days. The team’s dedication to quality, safety, and compassion has made a profound impact on patients and their families, making them truly deserving of this award.
East Dunbartonshire HSCP
Overall Winner Nominees
Innovation of the Year
Community Health and Care Services – Community Treatment and Care Service (CTAC) Team
The CTAC Team have been fundamental in the roll out of the programme for self-administration of B12 injections and have taught around 160 patients to take ownership of their long term condition. These patients have found that they have more independence and can receive their medication at a time that is more appropriate for them or they can have a friend or family member administer it (This person has been taught by CTAC staff). The aim of this innovation is to encourage patients to take over this aspect of their care and using values based conversations have given the patients independence and flexibility. These appointments will now be absorbed by the service and realigned to patients for other interventions or for those who are unable to self-administer.
Innovation of the Year
Tier 4 Child and Adolescent Mental Health Services (CAMHS) – Trauma Training Team
Clinicians across Tier 4 who were trained as trainers for the CAMHS NES Trauma Training package, and helped roll out this training across Tier 4 CAMHS as part of the CAMHS Pilot. Helped Tier 4 CAMHS services think about their practise and work towards becoming trauma informed services. Clinicians gave their time over 2 years to deliver the CAMHS NES Trauma Training package to all clinicians in Tier 4 CAMHS and deliver Sowing Seeds workshops to Business Support staff across Tier 4 and Hosted CAMHS services, as part of the CAMHS Pilot of this roll-out. In addition clinicians met with all Tier 4 CAMHS services to complete the Trauma Lens tool to help them think about their practise and develop a plan to further develop trauma informed practise in their services looking at: Choice, Collaboration, Safety, Trust and Empowerment. This was then reviewed with each services at the 2 year mark to evaluate the pilot and to help services develop a further plan to continue moving forward with trauma informed thinking and practise. Staff also provided Trauma Thinking Space groups for Tier 4 staff to allow for protected space to think about changes they might want to make and share practise across Tier 4. Clinicians adapted the NES Trauma Training Package, with approval and sign off from NES, to create a 1 day package to better meet the training needs of our inpatient staff and to allow for easier roll out when having to consider shift working. Clinicians supported senior staff to complete the Trauma Quality Improvement Framework to help thinking more widely about trauma informed practise. Considering HR policy, recruitment and wider service consideration such as paperwork, record keeping, standardised letters etc. All this was only possible due to the amazing support from Business Support in regards to keeping track of who attended training, printing out training packages and ensuring training days were well organised.
Innovation of the Year
Oral Health Directorate Lifelong Smiles Programme
This was an initiative designed to improve patient attendance at dental service appointments and increase the number of patients opting for alternatives to general anaesthesia.
This was a collaborative effort between the Public Dental Service, Children and Families, and Oral Health Improvement Teams aims to enhance both patient and staff experiences while reducing appointment waiting times.
Supported by Q Exchange funding the following was developed – Training for dental health support workers:
A new training package has been developed to educate young people and families about various treatment options.
This training includes practical elements and focuses on enhancing transferable skills such as active listening and collaborative decision-making with families.
Innovative information resources: To reduce dental anxiety and improve engagement, a package of information has been created for young people and families. This includes a series of four videos accompanied by written information, designed to prepare children and their parents or guardians for dental examinations, x-rays, and inhalation sedation.
Improved access and engagement: Families benefited from interactive sessions with team members at health centres, making it easier for them to access the care they need.
Further information on the main award categories
Team of the Year
The team, department, service or function that has been judged to have worked together as a team and made the most significant contribution to quality of care, population health and care, service delivery or staff wellbeing likely under significant pressure or difficult circumstances.
Employee of the Year
Any member of staff who has stood out as an exemplar of care giving, service delivery or who has made a major difference for colleagues around them or the delivery of a key objective for their department or wider NHSGGC/HSCP.
Leader of the Year
Any member of staff who has demonstrated outstanding leadership, positive values and behaviours and/or inspired others in a particularly challenging situation, or for the respect they get from others through the day to day difference they make for those around them as a leader.
Any member of staff can demonstrate leadership, not just those who formally manage people.
Innovation of the Year
To recognise any individual, team or department responsible for developing and implementing an innovative service, method, technology or process that has made a significant difference to quality of care, wider population health or care, service delivery or to the wellbeing of our own staff or to the efficient use our resources.
Volunteer of the Year
To recognise an individual or team of individuals who have volunteered significant time and effort to the benefit of our patients, service users or staff and made selfless contribution perhaps under difficult personal circumstances.
Was this helpful?
Yes
No
Thanks for your feedback!
The local staff awards are popular across all Directorates and HSCPs as they enable all areas to recognise and show appreciation to colleagues who have gone the extra mile. Everyone can give their own examples where amazing care or services have been delivered under hugely challenging conditions and staff have nominated the colleagues who they think most deserve recognition for their stand-out efforts, skills and commitment.
Presentations have been held in each local Directorate and HSCP to award the winners in categories including Employee of the Year, Team of the Year, Leader of the Year, Innovation of the Year and Volunteer of the Year, with the overall winners announced at the Celebrating Success Staff Awards Event on 28th May 2025.
You can find out more about each of the winners in each category below and about each of the nominees.
The winners were also announced live on the night on our social media channels (follow the #ggcawards hashtag).
Gautam was instrumental in setting up the Quality Improvement Den at the RAH in 2018. This opportunity has now been expanded to support colleagues across the Clyde sector.
The Den provides assistance and guidance for colleagues to pursue QI projects across a wide range of services, resulting in a skilled workforce and valuable improvements to patient care.
Cohort 7 is now underway, and over the years since the Den commenced, in excess of 127 colleagues have participated in it, delivering a broad range of improvement projects and encouraging a culture of continuous improvement across Clyde sector.
Acute Services – North Sector
Overall Winner – North Frailty Team
The North Frailty Team is a multidisciplinary group dedicated to improving care for older adults with frailty. Working alongside ED and AAU, they streamline patients to a specialist unit for timely Comprehensive Geriatric Assessments (CGA). Their innovative pathway has reduced the median length of stay from 16 to 11 days without increasing readmission rates. They introduced a CGA Huddle, integrating community teams to support early discharge.
Their commitment to person-centered care, collaboration, and overcoming resistance to change has enhanced hospital flow and patient outcomes. Patient feedback highlights their compassionate and high-quality approach, demonstrating that getting care right for older adults benefits everyone. Their dedication and teamwork make them truly deserving of this award.
Acute Services – South Sector
Overall Winner – Surgical Immediate Assessment Unit (IAU) , QEUH
The department is staffed by a combination of Healthcare Support Workers (HCSWs), Band 5 nurses, and Surgical Nurse Practitioners, with additional support from Advanced Nurse Practitioners (ANPs) and medical staff. This team works tirelessly to assess and implement the care needs of patients referred for surgical assessment by their GPs. They typically see a range of 730 to 750 patients per month and successfully discharge nearly half of them within four hours. Most discharges from the department occur between four and eight hours after arrival.
The team also runs Hot Clinics to ensure that patients do not remain in the hospital longer than necessary. If further tests are required, they arrange for patients to return for those procedures.
This exceptionally hardworking team deserves recognition for their contributions to unscheduled care.
Patient experience is significantly improved as most patients are seen within the four-hour target. Additionally, discharging patients to Hot Clinic slots reduces unnecessary waiting times for tests in an already busy department. This ensures that results can be discussed quickly after testing, allowing for effective further care planning.
The team is focused and driven, placing patients’ safety and well-being as their top priority.
Diagnostics
Overall Winner – Toxicology & Theraputic Drug Monitoring Service
Scottish drug-related deaths statistics show that drug misuse continues to be a significant problem. This has a direct impact on healthcare, including patients seeking help for drug use in primary care and hospital admissions across NHSGGC.
The Glasgow City Alcohol and Drug Partnership approached the QEUH Toxicology Team to discuss modernising drug screening; specifically, requesting an ability to detect a wider range of drugs.
As no commercial test kit was available to cover the range of drugs required, the Toxicology team developed a novel drug screen designed for local service users’ needs which was instrumental in the fight against drug-related deaths. Their innovation was a direct result of their ability to harness their collective brain power, knowledge, skills and experience to produce a transformative solution that benefited patients. The epitome of teamwork!
To date, over 14,000 patient samples have been screened using this test. A recent survey showed that service users agree that the extended screen they have developed has significantly improved patient management and had a positive impact on the population.
East Dunbartonshire HSCP
Overall Winner – Community Treatment and Care Service (CTAC) Team
Community Treatment and Care Service (CTAC) Team
The CTAC Team have been fundamental in the roll out of the programme for self-administration of B12 injections and have taught around 160 patients to take ownership of their long term condition. These patients have found that they have more independence and can receive their medication at a time that is more appropriate for them or they can have a friend or family member administer it (This person has been taught by CTAC staff). The aim of this innovation is to encourage patients to take over this aspect of their care and using values based conversations have given the patients independence and flexibility. These appointments will now be absorbed by the service and realigned to patients for other interventions or for those who are unable to self-administer.
East Renfrewshire HSCP
Overall Winner – Clair Blair
Claire is the ultimate champion for highlighting, advocating and supporting the health and wellbeing of the entire health and social care workforce.
Her kind, person-centred and empathetic personality helps bring people together. Claire has supported many colleagues through difficult times by being a listening ear, and sharing wisdom.
She also work in partnership with a number of organisations to support the delivery of wellbeing supports.
All of the judges were impressed by Claire’s ability to lead by example. She prioritises her own health and wellbeing, remaining resilient and positive, practices self-care, and makes use of wellbeing activities and resources.
eHealth
Overall Winner – eHealth and Clinical Teams involved in Ophthalmology Digital Patient Record
Commissioned by Scottish Government and in collaboration with clinical representatives from all Health Boards, eHealth National and Contractor Services, Information Management, Electronic Patient Record and Health Records teams worked together to develop and successfully implement the Ophthalmology Digital Patient Record and system.
This has been implemented across all NHSGGC Ophthalmology sites to connect primary and secondary eye care and enable transfer of patients between health boards. With the introduction of OpenEyes to NES Glaucoma Accredited Trained Community Optometrists, 749 patients have had their follow up care transferred to an Optometrist Practice near to their home.
Estates and Facilities
Overall Winner – Fiona Warnock-Greer
Fiona Warnock Greer, a Senior Project Manager within the Capital Planning team, has exemplified outstanding leadership through her management of the Parkhead Hub project, the largest primary care facility in the UK. Fiona’s dedication and teamwork have been instrumental in ensuring the project’s success, collaborating closely with diverse stakeholders, including HSCP, clinical areas, estates, facilities, design teams, contractors, and NHS Assure. Her leadership was particularly evident during the commissioning of the water system, where she established a short-life working group to ensure the highest standards were met. Fiona’s ability to navigate complex challenges, maintain clear communication, and foster a collaborative environment has been crucial in delivering a safe and functional facility.
Her proactive approach and commitment to excellence have earned her the respect and admiration of her colleagues. Fiona’s leadership has not only ensured the successful completion of the Parkhead Hub but also set a benchmark for future projects within the organisation.
Finance
Overall Joint Winners – The Payroll Team and SSTS
Payroll Team
Working above capacity to sustain services while delivering key additional activities, including multiple retrospective pay awards, new pension regulations, increased pension applications, partial retirement provisions, system updates, and controls from the Reduced Working Week.
SSTS
Ensuring no impacts on SSTS service provision, including increased activity from Reduced Working Week updates, while integrating the new eRostering system to normal business. This includes supporting early adopters, initial rollout and support at the IRH site, piloting medics at QEUH ED, and supporting the HIS pilot of Safe Care for Adult Mental Health Inpatient areas.
Glasgow City HSCP
Overall Winner – The Thistle Project Team
The Thistle Project Team has been recognised with Innovation of the Year for its groundbreaking role delivering the UK’s first Safer Drug Consumption Facility. Led by Glasgow City HSCP, this project brought together a range of partners, including Glasgow City Council, City Building, NHSGGC, and several others, to create a service that addresses complex health and social challenges.
The Thistle is a unique service, the implementation of which required innovative solutions to many service requirements never previously encountered within UK health environments. Through extensive consultations with Lived Experience Reference Groups and the surrounding community, the team ensured the facility was tailored to meet the unique needs of users, with the potential to significantly reduce harm and influence future legislation.
Human Resources & Organisational Development
Overall Winner – Mark Allen
Mark provides a fantastic administrative service to the Staff Governance Committee, Remuneration Committee and Workforce Equality Group.
Mark frequently supports other key initiatives within Staff Experience or across the broader HR Team, such as the EDI learning event or support for the Public Enquiry. In 2024, with the Head of HR Corporate leaving, Mark had to step in to lead much of the work around Remuneration Committee.
Gayle’s approach to recruitment ensured a team of dedicated individuals were introduced to the service to deliver support of varying intensities to meet the needs of each resident both in the Inverclyde Centre and in Temporary Furnished Flats in the community.
Gayle furnished a large communal lounge and a smaller lounge for outreach work, tirelessly engaged with third sector organisations and community assets to ensure residents received the care and attention of local dentists, opticians and student hairdressers who provided valuable services to make residents feel good about themselves.
She ensured they were trained in food hygiene to facilitate a brunch club three times a week providing wholesome and nutritious food to people who were hungry, and mentored residents in cooking and basic hygiene skills.
Pharmacy Services
Overall Winner – Primary Care Practice Educators
This programme, developed in 2023, was led by Tamara Cairney and delivered by dedicated Practice Educators across the HSCP teams. Over 2024, 53 pharmacists have been supported through the 12-week intensive period of supervision programme, beginning with a comprehensive Learning Needs Analysis.
This is aimed at developing pharmacists’ skills and confidence to manage increasingly complex patient care. This approach fosters the development of competence and autonomy, enhancing clinical decision-making capabilities. The program is designed to promote holistic professional growth by integrating reflective practice, patient feedback, and realistic clinical conversations. Pharmacists also have access to valuable well-being resources and are actively encouraged to collaborate within multidisciplinary teams, further enriching their learning experience.
Public Health
Overall Winner – Brian Laidlaw
Brian has demonstrated consistently his passion, commitment, and dedication to NHSGGC Hospital Support & Information Services (SIS) over the past 12 years. Recruited in April 2012, Brian has been a steadfast supporter of SIS frontline patient services, contributing weekly. His friendly, empathetic, and compassionate approach helps create a safe space for patients, carers, and families.
Brian balances the demands of healthcare volunteering with being a full-time carer for his wife. He is an integral part of the team, providing invaluable support to SIS workers and ensuring comprehensive care for patients and carers. NHSGGC SIS is proud to have him on their team.
Regional Services
Overall Winner – Magic Leap
This year’s Innovation prize went to staff at the Institute for Neurological Sciences who have been using a pioneering mixed reality (MR) system that allows them to “see inside” a patient’s body during surgery.
The MR goggles and system, known as the Magic Leap, are used by Consultant Neurosurgeon and Complex Spine Surgeon Mohamed Abdelsadg and colleagues to make surgeries less invasive and more accurate, minimising damage to other tissue.
The team were said to have “demonstrated remarkable dedication to advancing patient care by embracing cutting-edge technologies” that help to enhance precision.
Renfrewshire HSCP
Overall Winner – CIRCLE Recovery Hub
Challenging times with restructures and reduced finances in Renfrewshire have seen a reduction in Support staff at CIRCLE Recovery Hub with the referral rates continuing to be high.
Our support staff have continued to give everything they have to support individuals in Renfrewshire that have mental health and / or addiction related issues, by continuing to develop the service provision, not only within one building but a Recovery Community in Renfrewshire as a whole. The integrity of partnership working and seeing their provision as a piece of a large support network has supported these challenging times and also built strong connections with partner agencies, which aligns to future goals of the RHSCP.
West Dunbartonshire HSCP
Overall Winner – Gioia Sichi-Smith
As a key member of the West Dunbartonshire Alcohol and Drug Recovery Service, Gioia provides care, treatment and support to the most vulnerable people in the Community, making a difference every day.
Increasingly concerned at their lack of engagement with sexual health services, she completed additional training in this area of specialty, over and above her normal duties. Her qualifications have allowed her to commence a weekly Clinic which incorporates sexual health screening as well as other Harm Reduction interventions.
Collaborating with colleagues and services across West Dunbartonshire, Gioia is expanding this work further, promoting the benefits of regular healthcare, and delivering awareness training for service users to help them on their personal recovery journey.
A true inspiration to others!
Women & Children’s Services
Overall Winner – Neonatal Team, Royal Hospital for Children
The Neonatal team at RHC has been outstanding during a particularly challenging time of displacement from the Neonatal unit. Despite having their intensive care unit flooded, necessitating a move to another area of the hospital, the team continued to
provide high-quality care to extremely sick and preterm babies. Their dedication and compassion have been remarkable, making them truly deserving of recognition for their incredible efforts and resilience. The team has pushed above and beyond all reserves to deliver high standards of care.
Patients in the neonatal unit can be very unwell, and a few of them will not make the journey to go home. The team is helping families to create lasting memories, treating everyone with dignity and respecting their individual needs and backgrounds.
Further information on the main award categories
Team of the Year
The team, department, service or function that has been judged to have worked together as a team and made the most significant contribution to quality of care, population health and care, service delivery or staff wellbeing likely under significant pressure or difficult circumstances.
Employee of the Year
Any member of staff who has stood out as an exemplar of care giving, service delivery or who has made a major difference for colleagues around them or the delivery of a key objective for their department or wider NHSGGC/HSCP.
Leader of the Year
Any member of staff who has demonstrated outstanding leadership, positive values and behaviours and/or inspired others in a particularly challenging situation, or for the respect they get from others through the day to day difference they make for those around them as a leader.
Any member of staff can demonstrate leadership, not just those who formally manage people.
Innovation of the Year
To recognise any individual, team or department responsible for developing and implementing an innovative service, method, technology or process that has made a significant difference to quality of care, wider population health or care, service delivery or to the wellbeing of our own staff or to the efficient use our resources.
Volunteer of the Year
To recognise an individual or team of individuals who have volunteered significant time and effort to the benefit of our patients, service users or staff and made selfless contribution perhaps under difficult personal circumstances.
Was this helpful?
Yes
No
Thanks for your feedback!
Our dedicated teams and individuals were nominated for the prestigious NHSGGC Excellence Awards by patients, visitors and staff. All of our staff have gone above and beyond in the past year and we asked to hear about your experience of outstanding care and for your nominations.
There are 7 categories in our Excellence Awards and the winners were announced at the Celebrating Success Event on 28 May 2025.
The winners were announced live on the night on our social media channels (follow the #ggcawards tag).
You can find out who the Gold Winners were, read about the Silver Winners who were shortlisted, and also view photos and videos in each of the categories below.
Congratulations to all our winners!
Better Care
This award recognises staff who provide and contribute towards incredible patient care improving everyday practices across NHSGGC.
Gold Winner – Cancer Older People’s service
The Cancer Older Peoples Service at the Beatson has successfully established and implemented a comprehensive Occupational Therapy service which is specifically designed to support older cancer patients. It is the only service of its kind in Scotland and uses targeted interventions to significantly improve functional outcomes for patients, as well as supporting their health and wellbeing. The team also concentrates on ensuring safe discharge for patients from hospital, and the best ways to avoid unnecessary hospital admissions. They will undertake a thorough assessment of a patient’s physical, psychological, and social needs, while also incorporating age-specific screenings and interventions into routine cancer care.
Evaluation has shown positive improvements in clinical outcomes, patient satisfaction, and overall cost-effectiveness, with clear areas identified for further growth. The team is currently in discussion with other cancer centres across the country to share its framework, which has proven to be a highly transferable model.
Better Health
This award commends staff who have implemented an initiative to improve the health and wellbeing of patients, the public and/or staff.
Gold Winner – Tackling Health Inequalities for People Accessing the Pain Management Service
The Pain Management Service has recognised for a long time, significant health inequalities and barriers to access for patients with communication support needs. For non-English-speaking patients, language barriers often create significant challenges when navigating the healthcare system. This is particularly true in specialised services like pain management, where understanding treatment options and communication with healthcare providers is critical for successful outcomes.
The service made it their priority to break down these barriers and improve accessibility, ensuring that every patient has the support they need, in the language they understand. To help achieve this and informed by patient and staff feedback, the team launched a number of initiatives from revision of patient materials to incorporating pain management into interpreter training.
Better Value
This award is for staff who have increased efficiencies taking a new approach to work making better use of resources.
Gold Winner – North West Primary Care Pharmacy Team – Zendesk
Zendesk aimed to streamline community pharmacy queries to enhance patient care in the North West of Glasgow City. Utilising the platform, community pharmacies submitted queries online rather than by phone, allowing for quicker and more efficient handling. Key objectives included routing queries to appropriate pharmacy team members, reducing administrative workload in GP practices, and improving turnaround time for medication-related issues.
Launched in November 2024, the system handled 435 queries in two months, with 81% resolved by Pharmacy Support Workers, thereby freeing up over 60 hours of pharmacist capacity for face-to-face patient care. The initiative not only saved staffing costs—almost £850 in eight weeks—but also provided self-help resources for community pharmacies.
With expectations to handle over 15,000 queries annually, the project is set to release nearly 2,100 hours of pharmacist time and achieve annual savings of approximately £31,000. This innovative use of IT to direct workload enhances service efficiency and patient safety.
Better Workplace
This award recognises the often unseen work of our staff who help make NHSGGC a better workplace, improving the culture and supporting colleagues.
Gold Winner – Allied Health Professions Practice Education Team
The GGC Allied Health Professions (AHP) Practice Education Team aimed to enhance the educational experience for students and AHP staff within NHSGGC by implementing a multi-dimensional education programme. The AHP Director prioritises an inclusive education strategic framework for 12 healthcare professions, including AHP Health Care Support Workers (HCSW), ensuring access to innovative learning opportunities for the current and future workforce.
The Practice Education Team has played a pivotal role over the past two years by collaborating with key partners, improving communication, and designing new AHP educational opportunities. Their efforts have raised the profile of AHPs, transformed NHSGGC’s educational offerings, and supported career development for staff and students.
Key deliverables include enhancing practice-based learning placements, developing a funded modular programme in collaboration with Glasgow Caledonian University, and supporting HCSW workforce development through flexible programmes. The team also plays a vital role in staff support during the recovery renewal period, leading initiatives like the Return to Practice programme and promoting clinical skills through simulation.
Global Citizenship
This award recognises staff who have travelled overseas to provide healthcare and/or education in developing countries or countries in crisis.
Gold Winner – Gerry O’Hare and Dr Abdulla Alhasso
Breast Cancer Advanced Nurse Practitioner Gerry O’Hare and Dr Abdulla Alhasso, a Consultant Clinical Oncologist, bring a combined 20 years of experience in supporting cancer care in Palestine, with a particular focus on breast cancer in Gaza. Breast cancer outcomes for women in Gaza are significantly worse when compared to neighbouring countries and international benchmarks. Gerry and Abdulla have undertaken regular visits to Gaza over the past five years, which has been done in their own time and with the support of the Medical Aid for Palestinian organisation.
They collaborate with healthcare professionals in Gaza to enhance the clinical outcomes for women diagnosed with breast cancer by improving both their diagnosis and treatments. The pair also participate in weekly online multidisciplinary meetings with Palestinian colleagues to discuss optimal care for women presenting with early and advanced breast cancer, while also navigating the extremely challenging local circumstances.
Nursing and Midwifery
This award recognises nurse(s) who demonstrate the best qualities of patient care and the ethos of nursing.
Gold Winner – Brachytherapy Nursing Team
Nurses on the Beatson’s B3 ward are a highly specialised team helping to care for women with gynaecological cancers. They deliver brachytherapy, a type of radiotherapy that gives radiation inside the body and run the only nurse-led service in Scotland for women who require this treatment. The nurses pre-assess and examine patients and insert the necessary cylinders to allow patients to receive high dose radiation within a specialised unit.
This is a regional service for patients attending for sealed and unsealed sources of treatment. Melanie Whyte, Senior Charge Nurse, has been instrumental in helping to develop and implement the necessary protocols, safety advice and training for nurses in the unit. Patient feedback has confirmed patients attending the unit are happy with the service, and turnaround time has improved service delivery while also taking a huge time commitment away from Senior Consultants who previously carried out these treatments.
Volunteer
Recognising people who go the extra mile contributing tirelessly and providing outstanding help and support for the benefit of others.
Gold Winner – Morag Brierton, RAH volunteer
Morag is NHS Greater Glasgow and Clyde’s longest serving volunteer in acute services, having volunteered with the organisation for over 15 years. She is a Volunteer Driver for the Royal Alexandra Hospital Health at Heart team and transports patients to and from the hospital for cardiac rehab exercise classes in the Health at Heart gym. Within the service, patients also receive physiotherapy, education sessions, practical advice and emotional support, helping to rebuild their confidence and come to terms with a range of different heart conditions.
Transport within and around Renfrewshire to the hospital can be challenging, particularly for patients living in semi-rural areas. But Morag’s vital support helps break down barriers for patients – many of whom are older and at risk of isolation – in accessing the rehab programme. They enjoy spending time with Morag in the car having a chat, and she builds strong relationships with them over the weeks she is picking them up and taking them home.
Was this helpful?
Yes
No
Thanks for your feedback!
Introduction
The Care Home Education Facilitators (CHEFs) provide support to current and potential Practice Learning Environments (PLEs, clinical placements) for undergraduate student nurses. Non-NHS placements work with different governance and legislative system from the NHS and the CHEFs, therefore provide a more bespoke way of supporting nursing and care teams. Download our poster outlining the role of Care Home Education Facilitators, or visit NES Care Home Education Facilitator site for more details about the role.
Care homes can provide excellent learning opportunities for nursing students and students from a variety of other healthcare professions. In providing these learning experiences, they also expose these students to the possibility of a valued career in the care home sector and non-NHS settings on completion of their studies.
NHS Education England mapped all the NMC proficiencies and skills that students must achieve to various non-NHS placements. They created the guide below so students and practice supervisors can easily see all that they can achieve in a care home or similar placement.
Resources for care home Practice Supervisors and Practice Assessors
There are usually fewer Practice Supervisors (PS) and Practice Assessors (PA) in care homes than in NHS PLEs, and many PS are senior carers / nursing assistants rather than nurses. Our experience and feedback is that bespoke tools and resources are required to help and support these staff members in this role, as many don’t have other PS/PAs for immediate support. We offer additional support to non nurse PS on aspects of the NMC code, NMC role and the content of a nursing degree as many will be unfamiliar with this.
There are many other group and 1-to-1 sessions that CHEFs can support staff with in line with the national CHEF role descriptor and the Practice Education priorities:
General updates and support visits
PAD (completing the student paperwork)
An introduction to Future Nurse (proficiencies for ALL nurses) and SSSA (student supervision and assessment guidelines)
Registering and using the free Turas Learn online learning system & CHEF Turas learning catalogue.
The NMC Practice supervisor and Practice assessor roles – flexibility in practice examples.
Using the Turas professional portfolio for CPL, CPD and revalidation.
NMC Revalidation workshops
Working with students with competency or professionalism difficulties including creating development support plans DSP
Updating and using QMPLE (quality management system for practice learning environments)
The open university degree – awareness session
Signing off platform proficiencies and skills annexes in the PAD
Exploring complex proficiencies and skills for students
Supporting PS / PA to make reasonable adjustments for students (religion, disabilities, mental ill health etc.)
Completing the student final assessment and grading matrix.
Using the student activity “grab bags” as a resource
Creating a student welcome pack
Using the national pharmacology workbook with students
Using the Care Home placement workbook with students
Teaching of the entire practice supervisor / assessor content rather than it being self-directed – small 1-hour sessions over 6 weeks. (a quality improvement trial 2024-2025)
Placement resources that students should access
All information about individual care homes and similar placements is stored and accessible in the online platform QMPLE – the quality management of the practice learning environment website. The “suggested reading” section on QMPLE contains links to videos and resources that students should access prior to, and during their non-NHS placement. Please discuss with your CHEF if you would like QMPLE access as a care home staff member.
In order that students make the most of their Care home, or Non-NHS placements the CHEFs have devised these case studies – Case Study 1 and Case Study 2 to help give an overview of how your placement might work.
Example placement timetable
This example timetable will help you and your Practice Supervisors plan for learning and development opportunities. You can download a copy and modify for your own placement. We also have a blank copy of 8-week timetable for students available.
Care home workbook
Nationally, the CHEFs created a Care Homes Workbook which we advise all students to print off and complete during their placements, as this may provide evidence to practice supervisors and practice assessors of achieve proficiencies and skills.
Expectations of student and supervisors on care home placements
The below 3 links will indicate to you examples of care, nursing activities and behaviours expected of 1st, 2nd, and 3rd year students on placement, as well as a reminder of what to expect from supervisors and assessors
Lastly, these “Grab bag” activities were created so that if clinical activity is really busy or your supervisor (usually the only nurse or senior carer on duty) is called away to an urgent task which wouldn’t be appropriate for student learning; students can complete one of these activities, using evidence, research and local policy, and I relate it directly to the care of the residents in the clinical area.
Aside from facilitating student nurse education in care homes, we also provide bespoke education sessions for care home staff in a number of NHS Education for Scotland (NES) initiatives and useful development sessions.
At present we offer:
Flying Start NHS® – support for newly qualified nurses, or internationally educated nurses with a new NMC PIN.
Revalidation – requirements, planning, and using the Turas portfolio
The above links will provide general information on these programmes, but please contact your CHEF if you would like more information on bespoke provision within your care home or clinical environment.
Lastly, we wish to provide links to many other resources for care home staff to help in your own CPD, but also for the education of students and learners in practice:
We use cookies to analyse traffic to our site and to enable certain functions such as forms and YouTube videos. These do not collect personal information. By clicking "Accept All", you consent to our use of cookies, or you can customise the options.
This website uses cookies
Websites store cookies to enhance functionality and personalise your experience. You can manage your preferences, but blocking some cookies may impact site performance and services.
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
CloudFlare provides web performance and security solutions, enhancing site speed and protecting against threats.
Sequence rules uses cookies to track the order of requests a user has made and the time between requests and makes them available via Cloudflare Rules. This allows you to write rules that match valid or invalid sequences. The specific cookies used to validate sequences are called sequence cookies.
session
cf_ob_info
The cf_ob_info cookie provides information on: The HTTP Status Code returned by the origin web server. The Ray ID of the original failed request. The data center serving the traffic
session
cf_chl_rc_m
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
__cfruid
Used by the content network, Cloudflare, to identify trusted web traffic.
session
__cf_bm
Cloudflare's bot products identify and mitigate automated traffic to protect your site from bad bots. Cloudflare places the __cf_bm cookie on End User devices that access Customer sites that are protected by Bot Management or Bot Fight Mode. The __cf_bm cookie is necessary for the proper functioning of these bot solutions.
session
__cflb
When enabling session affinity with Cloudflare Load Balancer, Cloudflare sets a __cflb cookie with a unique value on the first response to the requesting client. Cloudflare routes future requests to the same origin, optimizing network resource usage. In the event of a failover, Cloudflare sets a new __cflb cookie to direct future requests to the failover pool.
session
_cfuvid
The _cfuvid cookie is only set when a site uses this option in a Rate Limiting Rule, and is only used to allow the Cloudflare WAF to distinguish individual users who share the same IP address.
session
cf_clearance
Whether a CAPTCHA or Javascript challenge has been solved.
session
cf_use_ob
The cf_use_ob cookie informs Cloudflare to fetch the requested resource from the Always Online cache on the designated port. Applicable values are: 0, 80, and 443. The cf_ob_info and cf_use_ob cookies are persistent cookies that expire after 30 seconds.
session
__cfwaitingroom
The __cfwaitingroom cookie is only used to track visitors that access a waiting room enabled host and path combination for a zone. Visitors using a browser that does not accept cookies cannot visit the host and path combination while the waiting room is active.
session
cf_chl_rc_i
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
cf_chl_rc_ni
These cookies are for internal use which allows Cloudflare to identify production issues on clients.