The Complex Mesh Surgical Service
This information is to help you know what you might be able to do in the days or weeks before any mesh related surgery. This will speed up your recovery and help you get the best outcome possible.
Even small positive changes in lifestyle make a difference and encourage you to be as healthy and strong as you can be.
Lifestyle changes that target your activity, weight and diet may help your bladder and bowel symptoms.
Being Active
Being active is one of the best things we can do for our physical and mental health.
Sometimes it can be hard to stay active when we have pain, leakage from the bladder or bowel, or struggle to find the motivation. Even small amounts of regular activity can make a difference.
The following tips might help:
- Start with small and regular activity that you enjoy and that is easy to do such as walking, or suitable exercise classes
- Try and find an exercise partner to help you stay motivated
- Plan to be active every day
- If you already go to classes, ask the instructor to help you with easier options for when you feel less strong or more uncomfortable
- Work towards increasing your daily activity over time
We know that physical activity can boost self-esteem, mood, sleep quality and energy.
The Government guidelines are shown below BUT not everything will suit everyone – get advice on the right strength training for you.
Managing your weight
A healthy weight is important for overall wellbeing and can help you prevent and control many diseases and conditions. National guidelines recommend that a body mass index (BMI) of less than 30 can help reduce symptoms of mixed urinary incontinence and prolapse. The link below will give you general information about the effects of a high BMI on your pelvic floor and the risk of complications during and after surgery.
Losing weight can be hard and you may need lots of help and support:
- Ask your friends to help you
- Speak to your GP
- Find out what is available locally
The links below may be useful:
Have a healthy balanced diet
What you eat and drink is very important for bladder and bowel health. Staying active also helps.
Fluids
It is important to drink enough each day even if you have bothersome bladder symptoms. Try to drink at least 1.5litres to 2litres of fluid per day. You may need to increase your fluids gradually to help retrain your bladder. It is recommended that you limit the amount of caffeine and fizzy drinks such as coke, coffee, energy drinks and alcohol because they are known to irritate the bladder.
Drinking enough may also help with constipation and encourage a regular bowel habit.
Food
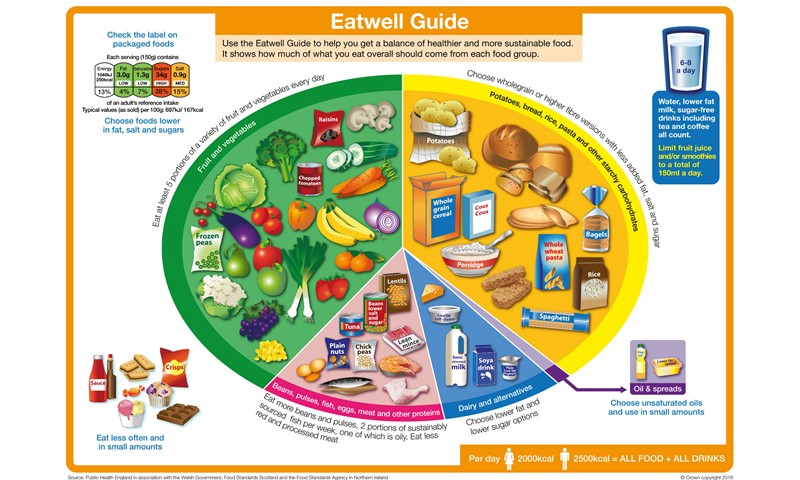
A balanced diet with enough fibre and physical activity can help to regulate your bowel movements, prevent constipation and improve rectal emptying. The right stool consistency may help manage symptoms of bowel urgency and leakage of poo.
Understanding how to have the right stool consistency is particularly important at the time of surgery to help prevent straining and constipation post operatively.
The Eatwell guide from the NHS gives an idea of what the balance of foods should be.
Further information and help is also available from the following links:
Other lifestyle modifications which may help manage pelvic floor symptoms
- Stopping smoking and managing any respiratory conditions such as asthma may reduce your cough. You may also feel fitter and more able to take part in physical activity. This in turn can benefit your mental health and wellbeing.
- Reducing alcohol intake. Alcohol is known to irritate the bladder. Other benefits of cutting down may be improved mood, sleep quality and feeling more energetic
For further help with this, see you GP for local services and have a look at the following website pages:
If your ability to make helpful lifestyle changes are not possible due to low mood, please seek help to find the right support for you.
Got a date for surgery?
Knowing what to expect from surgery can help reduce preoperative anxiety. The following link and short video will help to support and guide you:
You will also be seen ahead of your operation to get information on pre and post operative care.