As a new donor, you need to complete our screening process before donating. If you have stored milk, please complete the form for the period of the stored milk.
By completing the screening form, you agree that you have read the pre-screening information and:
Understand milk cannot be returned once donated
Consent to a sample of blood being tested for HIV, HTLV, Hepatitis B and C and syphilis
Consent to a positive blood result being shared with your GP
Consent to information about you, your health and donations being stored on a database
Consent to your milk being used for research purposes
We can’t accept milk from you if you:
smoke, or are using nicotine replacement therapy or are vaping
regularly drink more than 1 to 2 units of alcohol once or twice per week
take certain medications including antidepressants, high blood pressure medication and certain pain killers
We also ask that you keep your caffeinated drinks (tea, coffee, soft drinks) to a minimum.
Completing Donor Screening
Please answer the questions accurately as donation depends on the answers and the results of your blood tests. Answering yes doesn’t mean you can’t donate but we may need extra information.
As we can’t use antenatal blood results, we will send you a kit for a new blood sample to get taken at your GP practice. You post this back to us in a prepaid Royal Mail box. We test you for: HIV, Hepatitis B and C, HTLV 1 and 2 and Syphilis. We can give you more information on these tests if required.
If your blood test gives a positive result for any of these infections, we will refer you for advice on any issues which may affect your own health. A positive test means you can’t donate.
How long can I donate for?
It’s best to establish your own milk supply, usually around 6 weeks postnatally, before expressing for donation. You don’t need to express more than once a day and you can donate until your baby is around two.
Donations of already expressed milk are also accepted if the milk has been stored and frozen appropriately, is less than 90 days old and is a reasonable amount (around 3 litres or more).
Data Protection
The Milk Bank keeps a record of your information on a secure computerised database. This database is used to communicate with donors and to record your donation details, including your blood sample test results.
All your information is treated in the strictest confidence. Families whose babies receive donor milk can’t access your information at any point. Your information may also be used for research to improve our knowledge about the milk donor population, for clinical audit and to assess and improve the quality of our service. We may contact you for feedback on the service we provide.
We may use some of the information you give us for other reasons and sometimes the law requires us to pass on information if there is a genuine need (for instance in matters of Public Health). Whenever we can, we will remove details which identify you. All information and data that is processed by the Milk Bank is in accordance with the provisions of the Data Protection Act (1998). Everyone has a legal duty to keep all information confidential, and everyone who receives information from us is also legally obliged to keep it confidential. You have a right of access to your donor records. If you want to access your records, contact our Donor Coordinator.
Donor Screening Form
Once you have read all the information, please complete the screening form:
Your milk should be expressed by hand or breast pump. ‘Drip milk’ that leaks while you are feeding your baby from the other breast is not ideal as it tends to have less fat, protein and calories.
Your equipment for expressing does not need to be sterilised but good personnel hygiene, hand washing and clean preparation areas are important. Your expressing equipment should be washed in hot soapy water and clear of all milk debris, then rinsed in cool water, dried and stored in a container lined with paper towel and covered with a lid between uses. Please use paper towel for drying your hands and equipment.
We will provide sterilised collection bottles and labels for your milk. When collecting your milk, be careful not to touch the inside of the bottle or lid. Leave a 2cm gap at the top of the bottle as the milk will expand when frozen.
Where possible you should freeze your milk after expressing. If this is not possible, you can keep it in the fridge and frozen within 24 hours. It doesn’t matter if there is only a small amount of milk in a bottle at the end of each day. These can be topped up with chilled freshly pumped milk.
All your stored milk should remain frozen. We ask you to record the temperature of your freezer every day (preferably in the morning) and provide a thermometer for this. Store your milk in your freezer separately from food in the plastic bag we provide.
You should contact the milk bank staff to discuss donation if you:
develop a temperature or have been exposed to a virus that causes a rash such as chicken pox or German measles (rubella)
start taking medication
develop breast lesions or infections such as mastitis
travel outside the UK
Requesting Milk Collection
Remember milk must be processed within 90 days. You can request a collection and extra bottles and labels using the Milk Collection Form
Are incontinence pads provided for bodily fluids other than urine and faeces?
No. Incontinence pads are made differently to sanitary wear. Therefore they are not supplied for bodily fluids other than urine and faeces.
I’m in a wheelchair, will the clinic be accessible?
Most Health and Care Centres are accessible, but not all. Please contact us if you would like to discuss your individual access needs.
Why didn’t I receive an appointment nearer to home?
Please note that we don’t run clinics out of every Health and Care Centre across NHS Greater Glasgow and Clyde. We make every effort to give you an appointment near to home, but sometimes we might offer an earlier appointment at a venue a bit further away so you get seen sooner – please contact us if you have difficulty attending a particular venue and we will do our best to accommodate your needs.
Is it just my age?
Whilst age can be a factor in bladder and bowel control, there will be other reasons for your symptoms and age is not a barrier to successful treatment.
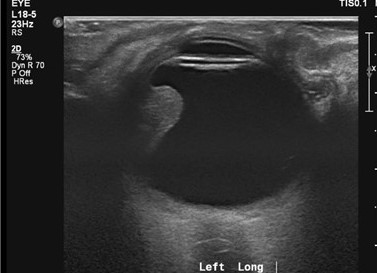
Why do you scan my bladder and what does the scan show?
We scan your bladder as part of our assessment to make sure it is emptying properly and make sure you get the right treatment.
Can my bladder or bowel symptoms be cured?
There is every likelihood that your symptoms can be improved and the possibility that they can be cured. That is why we ask you lots of questions about your bladder and bowel symptoms and examine you physically, check your urine and scan your bladder.
How do I access a urine sample container if I have nothing I can use at home?
You can get a urine sample container from your local pharmacy or GP surgery.
If I need a reassessment of my continence needs, how do I go about this?
You should contact your GP, who will make a re-referral.
What is a Behavioural Intervention Group (BIG)? Will I be expected to talk at it, or share any personal information? Will there be any men there?
The Behavioural Intervention Group consists of a small group of women. At this group one of our nurses will give you information about bladder symptoms and treatment options. You will not be expected to speak or to share personal information.
Why did you check my urine? What might show up and what does this mean?
We routinely test your urine to rule out any abnormalities, e.g. urinary tract infection. If we find anything abnormal we pass this to your GP for action.
Can I get pads?
Only after a thorough continence assessment, it may be necessary to prescribe pads for you. This is often only as a temporary measure whilst you are undergoing treatment.
Was this helpful?
Yes
No
Thanks for your feedback!
The NHSGGC SPHERE Bladder and Bowel Service provides a professional, caring, confidential and supportive approach to people with bladder or/and bowel symptoms.
The aim of the team is to treat bladder and bowel issues and also promote continence. By empowering the individual to self manage their symptoms, by teaching behavioural and lifestyle changes that can promote bladder and bowel health. To provide this support, the service has two specially trained teams across the city.
These teams include specialist nurses and physiotherapists who can advise and support the person on improving their bladder or/and bowel symptoms or prevent any deterioration by facilitating and providing rehabilitative treatments.
If you wish to be referred to our service and able to attend our clinic please contact your GP, who can arrange the referral for you.
Take the Continence Challenge to find out about your attitudes and beliefs towards continence.
How to reorder Incontinence Pads
Please be aware that Ontex customer service cannot amend prescriptions.
For anyone who has symptoms of bladder and/or bowel dysfunction, a referral can be made into the SPHERE Bladder and Bowel service by their GP.
It is the responsibility of the referrer to over-rule all red flags prior to referring into the SPHERE Service. These can be found within the relevant NICE guidelines below.
N.B. As per the Continence Referral Pathway, all housebound patients should be referred to the District Nurses initially for first level assessment and our team will support, should more specialist intervention be required.
This section summarises the different treatment options available for intraocular and extraocular tumours. After leaving clinic, you may have forgot to ask a question about the treatment advised. This is very common when being faced with a diagnosis of eye cancer. We hope this section will help answer your questions. Please see the different treatment options below.
Intraocular Tumour Treatments
Below is the list of treatments available to us for tumours that grow inside the eye. The most common tumour that grows inside the eye is melanoma. The most common treatment for this is plaque radiotherapy. If the tumour is too big for this treatment we may consider proton beam radiotherapy. We aim to select the best treatment suited to each patient as an individual. Unfortunately this sometimes means having to remove the eye (enucleation). Please see the different treatment options below.
Plaque Radiotherapy
Plaque radiotherapy is a form of internal radiotherapy. A radioactive piece of metal known as a plaque is attached to the sclera (white part of the eye) next to the tumour. This is around the size of a 5 pence coin (please see picture above). This is done in the operating theatre and is left in the eye between 3 and 7 days before being removed. Patients usually stay in ward 1C for this treatment. The tumour starts to shrink around 4-6 months after the plaque is removed.
The effects can last for several years. Although being an effective treatment, the radiation can sometimes damage other parts of the eye. This may cause cataract, retinal detachment, nerve damage, or macular oedema (swelling of the back of the eye). New blood vessels may grow after treatment; these can sometimes block the drainage angle in the eye causing glaucoma. If we are unable to control this, we may have to consider removing the eye. Although there are risks of plaque radiotherapy, this treatment can stop growth of the tumour in around 80% of cases.
Proton Beam Radiotherapy
This is where radiation with charged particles called protons are targeted at the tumour from outside the eye. This treatment is used if the tumour is too large or located too far back in the eye for plaque radiotherapy to work. As this treatment is highly specialised, the Douglas Cyclotron Unit, Clatterbridge, Liverpool is the only centre in the United Kingdom where the treatment is given.
If proton beam radiotherapy is the best option for you, we will organise transport to Clatterbridge and accommodation for you in near the Hospital (please see the team photo of the Clatterbridge team and the hospital above). This involves two separate visits to the Clatterbridge. At the first visit a treatment mask is made and fitted- this helps the team target the radiotherapy at the correct part of the eye. At the second visit, one to two weeks later, the treatment is given. You will likely travel down Sunday evening and return Friday later that week. Final measurements are made on the Monday and then the radiation is given over the remaining four days during (Tuesday to Friday).
Each treatment session takes around 20 minutes and is pain free. Before going down to Liverpool, however, we have to perform a small operation on the affected eye in Gartnavel General Hosptial, Glasgow. This is where we stitch tantalum markers (small metal discs smaller than a paper clip- please see photo above) to the sclera (white part of the eye) next to the tumour. We usually do this under General Anaesthetic. This helps the team target the radiation treatment more effectively when you go down to Clatterbridge. Proton beam radiotherapy takes a little longer to work than plaque radiotherapy.
We usually wait six months to see if the tumour starts to decrease in size. Although effective at treating tumours, the radiation can also damage normal parts of the eye and tissues around the eye when given. This may cause loss of eyelashes, loss of pigmentation of the eyelids, and inflammation of the conjunctiva causing a watery eye. Sometimes small blood vessels can grow at the back of the eye and into the drainage angle at the front of the eye. This can cause the pressure to build up in the eye and cause glaucoma. If we are unable to control the pressure and the eye becomes very uncomfortable, unfortunately we may have to consider removing the eye.
External Beam Radiotherapy
This is where radiation from a machine is targeted at cancer cells from outside the body. We find this treatment useful in patients that have cancer else where in the body that has spread to the back of the eye. On the other hand, if there has been a large tumour inside the eye that has grown behind the eye, we may choose to use radiotherapy after removing the eye. This treatment is spit into fractions.
This means the treatment is divided into smaller doses and spread out over a few days. This gives healthy cells in the body a chance to recover between treatments. If we are using radiation to treat the eyes or lymph nodes around the head and neck, then a special mask is usually made for patients. This mask is worn during treatment and helps aim the radiation at only the cancer cells. Although this helps prevent damage to healthy cells around the tumour, treatment may still cause loss of eyelashes, loss of pigmentation of the eyelids, and inflammation of the conjunctiva causing a watery eye.
Laser Transpupillary Thermotherapy
Transpupillary Thermotherapy (TTT) uses an infrared laser beam to heat the tumour up and kill the cancer cells. This technique is useful if there is uncertainty if the suspicious area is a melanoma or a naevus, or if the choroidal melanoma is small and radiotherapy is inappropriate due to poor health.
This treatment is sometimes combined with plaque radiotherapy as it reduces swelling and leakage from the blood vessels. After TTT the tumour gradually shrinks down if successful. Repeat treatment may be required at 6 months.
Possible complications from this treatment include retinal detachment, blockage of blood vessels, growth of new blood vessels, iris burns and cataract. Unfortunately tumour recurrence after treatment is common. This is more likely to occur if the melanoma is thick, close to the optic nerve, or non-pigmented.
Photo Dynamic Therapy
A light sensitive dye is injected into the blood stream. As the dye travels through the blood vessels to the back of the eye through the blood vessels, a special light is shined into the eye. This activates the dye and causes the abnormal blood vessels to close, shrink, and stop leaking.
This is useful in patients with a naevus or melanoma that is leaking fluid and building up at the back of the eye (macular oedema). Although this is not the main treatment for choroidal melanoma, we may find it useful in some cases where radiotherapy treatment is not possible.
Removal of Eye: Enucleation
Enucleation is the medical term for removing the eye. This is recommended when the tumour is too large for other treatments or has started to invade behind the eye. Removing the eye along with the tumour is sometimes preferred if there is a lot of pain and discomfort in the eye. This can be due to high pressure inside the eye caused by blockage of the drainage angle by tumour or new blood vessels grown after radiotherapy.
The idea of having your eye removed is scary. With current technology, however, we can get excellent cosmetic results with uniquely designed and fitted artificial eye implants (please click below to see photos). Our artifical eye clinic is run in Gartnavel General Hospital, Glasgow. Alternatively, some patients may prefer to just wear an eye patch after the tumour is removed.
After removing the eye, although this gets rid of the tumour growing in the eye, unfortunately this does not prevent the tumour growing else where in the body later in life. The most likely place for melanoma to regrow is the liver. For this reason we may decide to organise a liver ultrasound scan every year at your local hospital to screen for cancer growth.
Artificial Eyes
After the eye is removed, a temporary cosmetic shell is fitted in the operating theatre (see first picture above). We choose a colour to match the patient’s other eye. Although not a perfect colour match, this temporary shell will remain in place until the final artificial eye is made.
Once the eye socket has healed, the temporary cosmetic shell is removed and the final artificial eye implant can be fitted. This is done in the prosthetic eye department in Gartnavel General Hospital, Glasgow. The team will take photos of your normal eye. The artificial implant is then painted in fine detail to match the photo of your healthy eye. Please see the two other photos above (note both the healthy eyes have been dilated in clinic to examine the back of the eyes so the pupil sizes do not look symmetrical).
Removal of Eye and contents of Eye Socket- Exenteration
Exenteration means removing the eye with the tumour and the soft tissue around the eye. This treatment is required if the cancer has spread behind or around the eye. Sometimes the eyelids or part of the bone around the eye have to be removed if the tumour has invaded here. If this is the case, we will likely perform the operation at the Queen Elizabeth University Hospital with the help of our Oral and Maxilofacial Surgeon colleagues. Sometimes this treatment is combined with radiotherapy or chemotherapy. Our medical oncology team will help us choose the best treatment for you.
Excellent cosmetic results can be achieved after the tumour is removed. This involves further reconstructive surgery and being fitted with an artificial eye. Some patients, however, may prefer just to wear an eye patch or leave things as they are instead of having further surgery. After the cancer is removed we can plan treatment that suits your needs.
Extraocular Tumour Treatments
Please see below the list of treatment options for tumours that grow outside the eye. Every case is different. In clinic we will discuss the best treatment or combination of treatments for you.
Surgical Excision of Eyelid Tumours
This can be performed under local or general anaesthetic and as a day case. After tumour removal as much normal tissue is left behind to help keep the eyelid looking as normal as possible. The tumour is sent to the pathology laboratory to confirm the type of tumour and if it has all been removed. Eyelid tumours (mainly basal cell carcinomas) may be removed by a dermatologist (skin specialist). This is where a small part of the skin is removed then inspected under a microscope straight away. If cancer cells are still visible, then more tissue is removed and inspected again. This is repeated until there are no more cancer cells seen under the microscope. This helps remove as little normal tissue as possible mean while ensuring all the cancer is removed.
After the tumour is removed the eyelid is reconstructed to get the eyelid looking and functioning as normal as possible. If the tumour removed was small then this can usually be done on the same day. If the tumour removed was large and a lot of the eyelid had to be removed then reconstruction may be done on a different day. Skin or tissue can be taken from the other eyelid or from other parts of the body to re-form the eyelid. We commonly use the skin in front of the ear or from the inner surface of the upper arm. Sometimes we use tissue from the inner surface of the cheek- this heals very well after surgery. As there are many options, we aim to choose the best treatment option for you.
Freezing treatment: Cryotherapy
This freezes the tumour helping destroy the cancer cells. This can be used in combination with surgical excision, or on its own if surgery is not an option. Cryotherapy can is usually done the operating theatre under local or general anaesthetic. Treatment lasts several minutes. Although helping prevent tumour growth, no samples are sent to the lab so confirmation of tumour death is not always possible. If this is the case, we will monitor you carefully in the clinic. Sometimes we have to repeat this treatment more than once.
Radiotherapy
This treatment involves targeting the cancer with high energy radiation beams. This kills the cancer cells and stops them multiplying. This is used if surgery is not possible, for example, if the patient is too unwell or desperately does not want surgery. It may, however, be the preferred treatment of choice; for example, in lymphoma. This treatment is performed as an out-patient. This treatment is spit into fractions. This means the treatment is divided into smaller doses and spread out over a few days. This gives healthy cells in the body a chance to recover between treatments. If we are using radiation to treat the eyes or lymph nodes around the head and neck, then a special mask is usually made for patients. This mask is worn during treatment and helps aim the radiation at only the cancer cells. Although this helps prevent damage to healthy cells around the tumour, treatment may still cause loss of eyelashes, loss of pigmentation of the eyelids, and inflammation of the conjunctiva causing a watery eye.
Chemotherapy
Mitomycin C (MMC)
This is a chemotherapy drug that is applied to the surface of the tumour in theatre. MMC works by sticking the cancer cells’ DNA (the cell’s genetic code) together, stopping the tumour or cancer cells from growing.
This is applied to the surface of the cancer cells and therefore side effects of chemotherapy such as nausea, vomiting or hair loss are not experienced.
If MMC eye drops are being used, however, this can irritate the eye. We may give lubricant or steroid drops to treat this.
5-fluorouracil (5-FU)
This treatment, also called imiquimod, is a chemotherapy drug which is applied to the surface of skin tumours. Sometimes we use this to treat eyelid tumours. This drug causes the body’s immune system to produce a chemical called interferon. This attacks and kills cancer cells. It may irritate the skin when applied, this means the treatment is working. It is applied 3 – 5 nights a week and treatment can last up to 6 weeks.
Was this helpful?
Yes
No
Thanks for your feedback!
Our service is located in the:
Ophthalmology Out Patient Department Gartnavel General Hospital 1053 Great Western Road, Glasgow G12 OYN
Please click on “travel” below to help plan your journey. If you plan to travel the day before the clinic, please click on “accommodation” below.
Travel
We have bus and train links that travel to Gartnavel General Hospital daily.
Traveling by Train
Hyndland Station is the nearest train stop to Gartnavel General Hospital. We are a 5 to 10 minute walk from the Hyndland Station. Trains leave both Glasgow Queen Street Station and Glasgow Central Station every 10-15 minutes. The journey takes roughly 10 minutes to get to there. The following websites will help you plan your train journey if you are traveling from else where in Scotland:
Buses run frequently to from Glasgow City Centre to Great Western Road; this is a 5 minute walk to the main entrance to the hospital. Travel time may take up to 30 minutes during rush hour. The buses run every 10-15 minutes from the city centre. Please see the following links for time tables and to plan your journey:
When visiting family members on the ward, people who are elderly or live with a disability may find the evening hospital visitor transport service useful:
Parking is extremely limited at Gartnavel General Hospital. A maximum four hour stay operates in patient and visitor car parks from 7.30am until 4.30pm Monday to Friday. If there are no spaces, the Glasgow Pond Hotel next to Gartnavel General Hospital offer parking at reasonable rates. There is a designated drop off points outside all the entrances to the hospital. Please avoid parking on disabled spaces unless you hold a valid badge, and also taking care not to park on ambulance car parks or yellow lines.
Accommodation
We appreciate that patients and relatives may be travelling a long distance to attend the clinic. If you choose to travel the day before, Leonardos Inn Hotel is next to Gartnavel General Hospital. Please see their website for reservation and bookings.
Was this helpful?
Yes
No
Thanks for your feedback!
The Scottish Ocular Oncology Service is run by Dr Cauchi, Dr Chadha and Dr Connolly, experienced consultant ophthalmologists with a specialist interest in ocular oncology. Over the years we have a built up a close team of doctors , nurses, and non-medical staff from different backgrounds. These include:
Ophthalmologists (Eye doctors, both at consultant and registrar level)
Radiologists (Experts in CT, MRI, and Ultrasound scans),
Oncologists (Cancer specialists),
Pathologists (Experts in analysing tumours)
Specialist ophthalmic nurses (Nurses trained in counselling and able to answer questions about your diagnosis and treatment).
Anaesthetists (Experts at putting you to sleep for your operation)
Service Coordinators
Medical Photographers
Every Thursday morning we have our multidisciplinary team meeting (MDT). This is where we discuss patients who were listed for treatment the week before, and new patients coming to the clinic that day. Below are synopsis of the doctors and nurses from our team.
Ophthalmologists
Dr Cauchi
Dr Cauchi graduated from the Royal Free Hospital, University of London in 1996. His first interest in ophthalmology developed as a medical student, following in the footsteps of his grandfather who was also an ophthalmologist. He then did extra training in oculoplastics, orbits and ocular oncology. Dr Cauchi is one of the consultant ophthalmologists who run the Scottish Ocular Oncology Service.
Dr Chadha
Dr Chadha graduated from the University of Delhi in 1997 and underwent his basic and higher specialist training in ophthalmology at Edinburgh before doing a Fellowship in Ophthalmic Oncology and Oculoplastic Surgery at Glasgow in 2008-2009. He has been a Consultant in the West of Scotland since 2009 and is now one of the Consultants responsible for delivering the Scottish Ocular Oncology Service.
Dr Connolly
Dr. Julie Connolly started her career in academic research, completing her PhD from the University of Glasgow before undertaking further research roles in the Beatson Institute for Cancer Research. She subsequently graduated from University of Glasgow medical school before completing Ophthalmology specialty training and a fellowship in ocular oncology and oculoplastics in the West of Scotland Deanery. Dr Connolly is one of the consultants responsible for delivering the Scottish Ocular Oncology Service.
Oncologists
Dr Ritchie and Dr Schipani are the two Consultant Oncologists that work with the Scottish Ocular Oncology Service.
Dr. Schipani
Dr Schipani graduated from the University of Milan (Italy) in 2001. He underwent his Clinical oncology specialist training from 2002 to 2006, University of Milano-Bicocca (Italy) and worked as a consultant oncologist in Italy for three years. After taking a consultant job in Glasgow in 2009, Dr Schipani has developed a specialist interest in treating eye cancers and joined the Scottish Ocular Oncology Service team since September 2016.
Dr. Ritchie
Dr Ritchie after receiving her medical degree from Glasgow University started her clinical oncology training in 1986. She became a consultant oncologist in 1993 and has a specialist interest in radiotherapy treatment for eye cancers and skin tumours around the eye. She is one of the two consultant oncologists that help decide the correct treatment for patients with eye cancer.
Radiologists
Dr Cram is a consultant radiologist who has a specialist interest in Ocular Radiology. Below is the background of his career to date.
Dr Cram
Dr Cram graduated from St Andrews University in 2003 and received his medical degree from Manchester University in 2006. He decided to become at radiologist in 2007 and studied radiology in the West of Scotland Deanery. After becoming a full time consultant in August 2013 he is now one of the two Radiologists who work with the Scottish Ocular Oncology Service.
Pathologists
Dr Roberts and Dr Thum are both consultant pathologists that work with the Scottish Ocular Oncology Service. A summary of their experience to date is outlined below
Dr Roberts
Dr Roberts graduated from the University of Glasgow in 1991. During her training in general pathology she undertook a fellowship at the University of Illinois at Chicago undertaking research for her MD in ocular toxoplasmosis. On returning to Glasgow she completed her training in ophthalmic pathology under Professor William Lee before taking up a consultant position in 1998. She is a member and former secretary and president of the British Association of Ophthalmic Pathology and a member and former secretary of the European Ophthalmic Pathology society. In conjunction with Dr Thum she provides eye pathology input for the Scottish Ocular Oncology Service.
Dr Thum
Dr Thum graduated from medicine in Aberdeen in 2001. After years of practising ophthalmology, he decided to pursue a career in Pathology and started his training in Edinburgh in 2007. He became a consultant pathologist in 2015 and has been working with the Scottish Ocular Oncology Service for one year. Dr Thum is one of the two pathologists in our team who examine cells and tissue from tumour samples to help us select the best cancer treatment.
Nurses
Our team of nurses play an integral role in counselling and caring for patients throughout their diagnosis and treatment. Below is a summary of Agnes, Julie, Gayle and Nichola’s experience and training to date.
Agnes Macleod
Charge nurse Macleod trained in the Western Infirmary, receiving her nursing degree in 1989. She has been working with the Scottish Ocular Oncology Service team since 1994. Having had completed the Professional Studies Ophthalmic and Counseling Skills courses, she provides care and support to eye cancer patients attending the clinic and staying on the ward.
Gayle Williamson
Staff nurse Gayle Williamson trained in Stirling University and graduated from nursing in 2012. She has completed her post-graduate Eye course in 2018 and her counselling course in 2019. She has been part of the Scottish Ocular Oncology team since 2016 helping provide care and support to eye cancer patients attending the clinic.
Nichola Campbell
Staff nurse Nichola Campbell trained in Glasgow Caledonian University and graduated in 2010. She began working in the ophthalmology ward in 2012 and has been working with the ocular oncology team since 2014. She plays an integral role in seeing patients through their initial diagnosis, treatment, and post-operative care.
Fiona Wallace
Staff nurse Fiona Wallace trained in Edinburgh Napier University and graduated from nursing in 2003, she has completed her post-graduate Eye course in 2021. She has been part of the Scottish Ocular Oncology team since 2008 helping provide care and support to eye cancer patients attending the clinic.
Scientists
More information coming soon….
Service Coordinator
Susan Ewan
Susan Ewan is the service coordinator for the Scottish Ocular Oncology Service. She has been providing comprehensive secretarial and administrative support to the Scottish Ocular Oncology Service since June 2004. Susan is the main point of contact for Health Professionals and patients alike. She arranges new appointments, scans and any treatments that may be required along with travel arrangements and transfer of information to the Douglas Cycloton Unit for patients having proton beam therapy.
Was this helpful?
Yes
No
Thanks for your feedback!
For referrals please address letter to Dr Cauchi, Dr Chadha or Dr. Connolly at the following address:
Scottish Ocular Oncology Service Ophthalmology Out Patient Department Gartnavel General Hospital 1053 Great Western Road Glasgow G12 OYN
National Services Division Scottish Ocular Oncology Service
These guidelines are not intended to be prescriptive but to act as an aid to considering referral of patients to the nationally designated ocular oncology centre in Scotland at Gartnavel General Hospital. Glasgow.
Referring ophthalmologists should continue to exercise discretion based on the individual clinical presentations of their patients.
1. Whom to refer to the service
1.1 Patients with intraocular tumours
Any primary intraocular tumour other than naevus
Any intraocular metastatic tumour if specialist ocular oncology is required
Suspected intraocular lymphoma.
1.2 Patients with conjunctival and epibulbar tumours that appear invasive
1.3 Refer patient with conjunctival melanocytic tumour if :
Diameter exceeds 3 mm, especially in absence of clear cysts.
1.4 Patients with a suspicious melanocytic choroidal tumour having:
A: One of the following:
Thickness greater than 2.0 mm
Collar-stud configuration
Documented growth
B: Two of the following:
Thickness > 1.5mm
Orange pigment
Serous retinal detachment
Symptoms.
1.5 Refer patient with an iris nodule if:
Tumour is more than 3.0 mm in diameter
Tumour is markedly elevated
Secondary glaucoma or cataract
Tumour involves angle.
1.6 Patients with adnexal and orbital tumours if:
Eyelid tumour where ulceration and lash loss are evident or recurrence has occurred
Orbital tumours.
2. Whom not to refer to the service
2.1 Congenital hypertrophy of retinal pigment epithelium
2.2 Simple naevi, if:
Small and flat, or
Minimally raised with only drusen on the surface
Referral Form for Ophthalmologists
Please complete the referral form below and send it along with your referral letter. We would be grateful if these could be emailed along with any images, OCT or ultrasound scans.
Below are a list of publications produced by our department. We aim to continue producing good quality research to improve patient care.
Shams F, Cauchi P. Lagophthalmos and Ptosis in Inclusion Body Myositis. Ophthal Plast Reconstr Surg. 2016 Jan 18. [Epub ahead of print] PubMed PMID: 26784549.
Chia SN, Smith HB, Kemp EG. Comment on: ‘Pars plana vitrectomy to repair retinal detachment following brachytherapy for uveal melanoma’. Br J Ophthalmol. 2014 Apr;98(4):571. doi: 10.1136/bjophthalmol-2013-304749. PubMed PMID: 24390168.
Jamison A, Gregory ME, Lyall DA, Kemp EG. Visual outcomes following orbital biopsy. Orbit. 2013 Oct;32(5):304-8. doi: 10.3109/01676830.2013.814688. PubMed PMID: 23895509.
Cloke A, Lim LT, Kumarasamy M, Roberts F, Kemp EG. Lymphomatoid papulosis of the eyelid. Semin Ophthalmol. 2013 Jan;28(1):1-3. doi: 10.3109/08820538.2012.680643. PubMed PMID: 23305430.
Galea M, Cauchi P, Kemp E. Diode laser thermotherapy for conjunctival vascular malformations. Clin Exp Ophthalmol. 2013 Apr;41(3):307-8. doi: 10.1111/j.1442-9071.2012.02878.x. PubMed PMID: 22957708.
Irvine F, Kumarasamy M, Kemp E, Roberts F. Progression of primary acquired melanosis with atypia during pregnancy. Arch Ophthalmol. 2012 Aug;130(8):1085-7. doi: 10.1001/archophthalmol.2012.422. PubMed PMID: 22893092.
Achtsidis V, Gregory ME, Roberts F, Kemp EG. Enophthalmos following orbital trauma: a diagnostic catch. Br J Ophthalmol. 2012 Sep;96(9):1268-9, 1277. doi: 10.1136/bjophthalmol-2012-301996. PubMed PMID: 22872674.
Obi EE, Drummond SR, Kemp EG, Roberts F. Pleomorphic adenomas of the lower eyelid: a case series. Ophthal Plast Reconstr Surg. 2013 Jan-Feb;29(1):e14-7. doi: 10.1097/IOP.0b013e31825b34c1. PubMed PMID: 22743699.
Galea M, Falzon K, Chadha V, Williams G. Presumed occult globe rupture resulting in sympathetic ophthalmia. J Ophthalmic Inflamm Infect. 2012 Sep;2(3):137-40. doi: 10.1007/s12348-011-0056-4. PubMed PMID: 22200914; PubMed Central PMCID: PMC3438300.
Li Yim JF, Sandinha T, Kerr JM, Ritchie D, Kemp EG. Low dose orbital radiotherapy for thyroid eye disease. Orbit. 2011 Dec;30(6):269-74. doi: 10.3109/01676830.2011.615455. PubMed PMID: 22132844.
Wong KK, Roberts F, Cauchi P, Diaper C. Caliber persistent artery of the eyelid. Graefes Arch Clin Exp Ophthalmol. 2011 Sep;249(9):1395-7. doi: 10.1007/s00417-011-1685-x. PubMed PMID: 21494872.
Livingstone I, Ramamurthi S, Drummond S, Kemp E, Roberts F. Corneal perforation due to limbal involvement in Sézary syndrome. Graefes Arch Clin Exp Ophthalmol. 2011 Jul;249(7):1091-4. doi: 10.1007/s00417-010-1611-7. PubMed PMID: 21253759.
Macdonald EC, Cauchi P, Kemp EG. Proton beam therapy for the treatment of uveal melanoma in Scotland. Br J Ophthalmol. 2011 Dec;95(12):1691-5. doi: 10.1136/bjo.2010.195594. PubMed PMID: 21216794.
Obi EE, McDonald A, Kemp E. A bilateral cicatricial ectropion and bilateral upper lid shortening caused by 5-fluorouracil toxicity in a patient with dihydropyrimidine dehydrogenase deficiency. Cutan Ocul Toxicol. 2011 Jun;30(2):157-9. doi: 10.3109/15569527.2010.532846. PubMed PMID: 21077799.
Lim LT, Agarwal PK, Cauchi P, Diaper CJ. Laterality of periocular basal cell carcinomas in relation to driving practices in Scotland, United kingdom. Ophthal Plast Reconstr Surg. 2011 Jul-Aug;27(4):306. doi: 10.1097/IOP.0b013e3181f9e04b. PubMed PMID: 21057343.
Gregory ME, Chadha V, Roberts F, Kemp EG, Cauchi PA. Bilateral central retinal artery occlusion in a patient with primary central nervous system lymphoma. Graefes Arch Clin Exp Ophthalmol. 2011 Aug;249(8):1269-70. doi: 10.1007/s00417-010-1541-4. PubMed PMID: 20963435.
Lockington D, Chadha V, Russell H, Cauchi P, Tetley L, Roberts F, Kemp E. Histological evidence of tissue reaction to gold weights used for mechanical ptosis. Arch Ophthalmol. 2010 Oct;128(10):1379-80. doi: 10.1001/archophthalmol.2010.235. PubMed PMID: 20938017.
Lockington D, Chadha V, Russell H, Young D, Cauchi P, Kemp E. Socioeconomic status and choroidal melanoma in Scotland. Arch Ophthalmol. 2010 Mar;128(3):383-4. doi: 10.1001/archophthalmol.2009.407. PubMed PMID: 20212216.
Gonzalez P, Kemp EG, Roberts F. Recurrent choroidal melanoma after transscleral local resection with diffuse vitreous seeding. Graefes Arch Clin Exp Ophthalmol. 2010 May;248(5):741-6. doi: 10.1007/s00417-009-1261-9. PubMed PMID: 20127353.
Drummond SR, Kemp EG. Successful medical treatment of blepharochalasis: a case series. Orbit. 2009;28(5):313-6. doi: 10.3109/01676830903071190. PubMed PMID: 19874128.
Aziz S, Taylor A, McConnachie A, Kacperek A, Kemp E. Proton beam radiotherapy in the management of uveal melanoma: Clinical experience in Scotland. Clin Ophthalmol. 2009;3:49-55. PubMed PMID: 19668544; PubMed Central PMCID: PMC2708985.
Borooah S, Chadha V, Sutherland S. A case of permanent retinal disturbance postpartum following administration of ergometrine. Can J Ophthalmol. 2008 Oct;43(5):607-8. doi: 10.3129/i08-096. PubMed PMID: 18982049.
Ross JJ, Dean SJ, Koppel DA, Roberts F, Kemp EG. Massive orbital recurrence of uveal melanoma without metastases after 28 years. Br J Ophthalmol. 2010 May;94(5):632. doi: 10.1136/bjo.2008.146340. PubMed PMID: 18971235.
Ross JJ, Kemp EG. Large choroidal osteoma with macular decalcification. Retina. 2009 Mar;29(3):413-4. doi: 10.1097/IAE.0b013e3181871c2a. PubMed PMID: 18784621.
Chadha V, Cruickshank I, Swingler R, Sanders R. Advanced glaucomatous visual loss and oral steroids. BMJ. 2008 Aug 1;337:a670. doi: 10.1136/bmj.a670. PubMed PMID: 18676441.
Cauchi PA, Ang GS, Azuara-Blanco A, Burr JM. A systematic literature review of surgical interventions for limbal stem cell deficiency in humans. Am J Ophthalmol. 2008 Aug;146(2):251-259. doi: 10.1016/j.ajo.2008.03.018. Review. PubMed PMID: 18486098.
Henriquez F, Janssen C, Kemp EG, Roberts F. The T1799A BRAF mutation is present in iris melanoma. Invest Ophthalmol Vis Sci. 2007 Nov;48(11):4897-900. PubMed PMID: 17962436.
Dean SJ, Ross J, Kemp E. Bilateral spontaneous idiopathic extraocular muscle haematoma. Clin Exp Ophthalmol. 2007 May-Jun;35(4):369-71. PubMed PMID: 17539791.
Chadha V, Barr A. Rare ocular and systemic associations in a case of neurofibromatosis 2. J Pediatr Ophthalmol Strabismus. 2007 Mar-Apr;44(2):124-6. PubMed PMID: 17410965.
Chadha V, Borooah S. Variations in intake of tamsulosin. J Cataract Refract Surg. 2007 Mar;33(3):362-3. PubMed PMID: 17321374.
Cauchi PA, Sarros M, Atta HR. Deposition of triamcinolone crystals on the posterior lens capsule following prone posturing post-vitrectomy. Acta Ophthalmol Scand. 2006 Dec;84(6):828. PubMed PMID: 17083550.
Sandinha T, Russell H, Kemp E, Roberts F. Malignant melanoma of the conjunctiva with intraocular extension: a clinicopathological study of three cases. Graefes Arch Clin Exp Ophthalmol. 2007 Mar;245(3):431-6. PubMed PMID: 16941140.
Chadha V, Pandey PK, Chauhan D, Das S. Simultaneous intraocular and bilateral extraocular muscle involvement in a case of disseminated cysticercosis. Int Ophthalmol. 2005 Feb-Apr;26(1-2):35-7. PubMed PMID: 16779570.
Cacciatori M, Chadha V, Bennett HG, Singh J. Trypan blue to aid visualization of the vitreous during anterior segment surgery. J Cataract Refract Surg. 2006 Mar;32(3):389-91. PubMed PMID: 16631044.
Cauchi P, Azuara-Blanco A, McKenzie J. Corneal toxicity and inflammation secondary to retained perfluorodecalin. Am J Ophthalmol. 2005 Aug;140(2):322-3. PubMed PMID: 16086960.
MacAndie K, Kemp E. Impact on quality of life of botulinum toxin treatments for essential blepharospasm. Orbit. 2004 Dec;23(4):207-10. PubMed PMID: 15590520.
Ooi KG, Drummond SR, Thompson KJ, Roberts F, Kemp EG. Churg-Strauss syndrome presenting with conjunctival nodules in association with Candida albicans and ankylosing spondylitis. Clin Exp Ophthalmol. 2004 Aug;32(4):441-3. PubMed PMID: 15281986.
Gear H, Williams H, Kemp EG, Roberts F. BRAF mutations in conjunctival melanoma. Invest Ophthalmol Vis Sci. 2004 Aug;45(8):2484-8. PubMed PMID: 15277467.
Pandey PK, Narayanan R, Chaudhuri Z, Chadha V, Jain S. An unusual case of neurofibromatosis fulfilling the diagnostic criteria for types I and II. J Pediatr Ophthalmol Strabismus. 2002 Sep-Oct;39(5):313-6. PubMed PMID: 12353908.
Muscat S, McKay N, Parks S, Kemp E, Keating D. Repeatability and reproducibility of corneal thickness measurements by optical coherence tomography. Invest Ophthalmol Vis Sci. 2002 Jun;43(6):1791-5. PubMed PMID: 12036980.
Muscat S, Parks S, Kemp E, Keating D. Repeatability and reproducibility of macular thickness measurements with the Humphrey OCT system. Invest Ophthalmol Vis Sci. 2002 Feb;43(2):490-5. PubMed PMID: 11818395.
Was this helpful?
Yes
No
Thanks for your feedback!
We have a several tests available to us to help us diagnose your condition and to help us decide on the best treatment. For choroidal melanoma, the most common type of eye cancer we see in our clinic, we routinely perform ultrasound scan of the eye in our radiology department. This is usually done before being seen in the eye clinic. Please see a list of investigations we may use below.
Ultrasound Scan
An Ultrasound scan is often used in pregnancy and uses sound waves to create an image of inside a part of the body. It is very safe and can look at organs in the abdomen, for example the liver, or of the eye. Either a doctor or a sonographer (health professional trained to perform ultrasound scans) will perform the scan. You may be asked to follow certain instructions before your scan- such as drinking a lot of water, fasting for a few hours etc- it is important you try and follow these instructions to get the best images possible. Cold gel is applied to the skin over the area they wish to scan.
The ultra-sound probe is gently placed on the skin and moved over the gel. If the eye is being scanned, the ultrasound probe is gently applied to the surface of the eyelid. The ultrasound images are then collected and analysed. Ultrasound scans of the body may take between 15-45minutes to perform. Ultrasound of the eye, however, is much quicker and will sometimes be performed in the eye clinic. Results of the eye USS will be given on the same day. Results of liver ultrasound scans, if carried out your local hospital, will be discussed at your next eye clinic appointment.
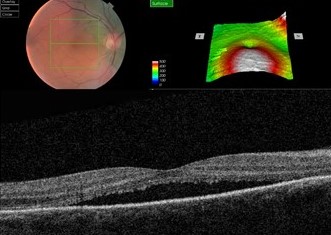
Optical Coherence Tomography (OCT)
This is a large camera, which creates 3D pictures of the back of the eye. After having your pupils dilated with drops, the scan takes minutes to perform. This helps us check for fluid leaking at the back of the eye from abnormal blood vessels or from a tumour. It can be repeated at each visit, and helps us pick up changes at the back of the eye.
CT Scan
CT scans are also known as CAT scans. They use several X-ray images to create a detailed scan of the body. When you arrive at the department you will have a short safety questionnaire to complete; due to radiation CT scans are not usually recommended in women who are pregnant. Sometimes contrast dye is injected into the vein during the scan to help get more detailed images.
The CT scanner itself is a large circular machine, which you lie flat in. You will be asked to stay still and breathe normally. The x-ray parts move inside the big circular ring creating the images. During the scan, you will be able to communicate with the radiographer in the next room through an intercom system. The scan takes around 10 to 20 minutes to do. After the scan, the images are analysed and the results will be given to you at your next clinic appointment.
MRI Scan
Add/copy info from UmbMRI stands for magnetic resonance imaging. Instead of X-ray radiation, It uses magnets and radio waves to produce images of inside the body. It gives very fine detailed pictures of the eye, the optic nerve, and the brain. When you arrive at the department you will have a short safety questionnaire to complete; if you have any metal inside the body or are claustrophobic you may not be able to get the MRI scan. Sometimes contrast dye is injected into the vein during the scan to help get more detailed images.
The MRI scanner is a large circular tube, which you lay down flat in. The radiographer then leaves the room to operate the scanner from the next room. You will be able to communicate with them however through an intercom system. During the scan you will be asked to lie still and to breathe normally. You may hear loud tapping noises during the scan- this is normal. You will be given earplugs or headphones to wear so you can listen to music. The scan takes 30 minutes to an 1 hour to complete. After the scan, the images are analysed and the results will be given to you at your next clinic appointment.
Chest X-Ray
X-rays are used to produce pictures of the heart, lungs and other parts of the body. This is quick to perform in the radiography department and is useful if we want to check for lung cancer.
Fundus Fluorescein Angiography (FFA)
This is where a yellow dye is injection into a vein in the arm, which travels through the blood vessels to the back of the eye. As the dye reaches the back of the eye, several pictures are taken with a special camera. This gives us more information about the blood supply to suspicious areas at the back of the eye.
Indocyanide Green Angiography (ICG)
This is similar to fluorescein angiography, except a different dye is used. This looks more closely at the choroid at the back of the eye, which is the layer deeper to the retina. It is therefore useful at detecting abnormalities in the blood vessels in the choroid.
We use cookies to analyse traffic to our site and to enable certain functions such as forms and YouTube videos. These do not collect personal information. By clicking "Accept All", you consent to our use of cookies, or you can customise the options.
This website uses cookies
Websites store cookies to enhance functionality and personalise your experience. You can manage your preferences, but blocking some cookies may impact site performance and services.
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
CloudFlare provides web performance and security solutions, enhancing site speed and protecting against threats.
Sequence rules uses cookies to track the order of requests a user has made and the time between requests and makes them available via Cloudflare Rules. This allows you to write rules that match valid or invalid sequences. The specific cookies used to validate sequences are called sequence cookies.
session
cf_ob_info
The cf_ob_info cookie provides information on: The HTTP Status Code returned by the origin web server. The Ray ID of the original failed request. The data center serving the traffic
session
cf_chl_rc_m
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
__cfruid
Used by the content network, Cloudflare, to identify trusted web traffic.
session
__cf_bm
Cloudflare's bot products identify and mitigate automated traffic to protect your site from bad bots. Cloudflare places the __cf_bm cookie on End User devices that access Customer sites that are protected by Bot Management or Bot Fight Mode. The __cf_bm cookie is necessary for the proper functioning of these bot solutions.
session
__cflb
When enabling session affinity with Cloudflare Load Balancer, Cloudflare sets a __cflb cookie with a unique value on the first response to the requesting client. Cloudflare routes future requests to the same origin, optimizing network resource usage. In the event of a failover, Cloudflare sets a new __cflb cookie to direct future requests to the failover pool.
session
_cfuvid
The _cfuvid cookie is only set when a site uses this option in a Rate Limiting Rule, and is only used to allow the Cloudflare WAF to distinguish individual users who share the same IP address.
session
cf_clearance
Whether a CAPTCHA or Javascript challenge has been solved.
session
cf_use_ob
The cf_use_ob cookie informs Cloudflare to fetch the requested resource from the Always Online cache on the designated port. Applicable values are: 0, 80, and 443. The cf_ob_info and cf_use_ob cookies are persistent cookies that expire after 30 seconds.
session
__cfwaitingroom
The __cfwaitingroom cookie is only used to track visitors that access a waiting room enabled host and path combination for a zone. Visitors using a browser that does not accept cookies cannot visit the host and path combination while the waiting room is active.
session
cf_chl_rc_i
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
cf_chl_rc_ni
These cookies are for internal use which allows Cloudflare to identify production issues on clients.