To arrange a collection of milk, please complete the form below and submit by Wednesday with your availability for the following week.If the form is submitted between Thursday and Sunday availability would be for the next week again.
Our volunteers all carry personalised identification cards. The service has a doorstop policy and volunteers will not enter your home. The only exception to this would be if you have an accessibility requirement and were unable to bring the milk to the door yourself. On these occasions our volunteers will carry out a personal risk assessment before entering your home, for example finding out if the household has a pet before offering assistance.
We will be in touch shortly to let you know when we will be out.
If you need a freezer sheet you can download it by clicking the following link.
Pre-op Assessment Department is situated within the main hospital building, Clinic K Level 2. To access pre op assessment enter via the main entrance. Take the lift to level 2 – come out the lift and turn left. Walk along the corridor until you come to Clinic K.
There are 3 car parks within the hospital grounds. There is no charge for parking within the hospital grounds.
Getting to New Stobhill Hospital by Public Transport
First 3: from/to – City Centre, Hope Street – Springburn – Stobhill Hospital
Henderson Travel 329: from/to – City Centre, West Regent Street – Roystonhill – Springburn – Stobhill Hospital
First 31: from/to Milton – Springburn – Royal Infirmary – City Centre, Stockwell Street – Castlemilk – East Kilbride, Lindsayfield
First 45: from/to Auchinairn – Springburn – Sighthill – City Centre, Union Street – Shawlands – Kennishead
First 88: from/to Harestanes – Bishopbriggs – Springburn – St Rollox – Buchanan Bus Station
Henderson Travel 71: from/to Torrance – Bishopbriggs – St Rollox – Buchanan Bus Station
Henderson Travel 72: from/to Kirkintilloch – Robroyston – Springburn – Cowcaddens – Buchanan Bus Station
Henderson Travel 271: from/to to Torrance – Bishopbriggs R – Cowcaddens – Buchanan Bus Station
Below are local directions to the hospital, followed by directions for motorway travellers. If using a SatNav or similar device, use the postcode G21 3UW to obtain directions.
Cowcaddens and Royston – use Springburn Road A803, go straight through two sets of traffic lights, and proceed for one mile, turning right after the petrol station into Stobhill Road. Then go straight over at traffic lights on to the approach road of the hospital grounds.
Maryhill – from Maryhill Road, turn left into Bilsland Drive. At the traffic lights, go straight over into Hawthorn Street, turn left at the end of the street into Balgrayhill Road and turn right into Belmont Road, which leads into the hospital.
Balornock and Barmulloch – use Broomfield Road and Balornock Road, turning left into the hospital at the end of Springburn Park.
Dennistoun and east end of city – use Alexandra Parade, turning right into Castle Street at Glasgow Royal Infirmary and left into Baird Street. Take the first right for Springburn Road A803 until you reach Stobhill Road and then continue as above.
Bishopbriggs and Kirkintilloch – use Kirkintilloch Road A803, then turn left into Colston Road. Take the right hand lane at the mini-roundabout into Balgrayhill Road, then first left into the hospital.
Motorway Travellers
M8 from West exit junction15 and follow signs for Kirkintilloch, A803 (Springburn Road). Using the A803, go straight through two sets of traffic lights. Proceed for one mile, turning right after the filling station (Stobhill Road).
M8 from East exit Junction 15, turn right at traffic lights, left at next lights and follow road to join A803 and follow as above.
M80 exit Junction 2 and follow signs for B765 Bishopbriggs. At the supermarket roundabout take third exit. Next roundabout take first exit, ‘Local’. Next roundabout take third exit. Take first left onto Wallacewell Road. Go straight through roundabout, at end of road turn right into Balornock Road. Turn left into hospital grounds at end of Springbun Park.
Cafés
Aroma café Ground Floor New Stobhill Hospital – Open Monday to Friday 8.00am to 5.00pm
Aroma Plus 3rd Floor: Open Monday to Friday 8.00am – 5.00pm
Plastic Surgery Pre-operative assessment Plastic Surgery Outpatient department Glasgow Royal Infirmary 84 Castle street, G4 OSF
Car Parking
There is a multi-story carpark within the hospital grounds (there is no charge for this carpark) There is multiple carparks around the hospital site, off High Street and on Wishart Street, these are private car parks and charge for parking.
Cafes/Canteens
The Little Royal Cafe (not NHS owned) is located next door to the Plastic Surgery Out Patient building, the hospital has 2 canteens, 1 situated in the Centre block and the Campsie restaurant in the basement of the Queen Elizabeth Building, there is an Aroma coffee shop within the main Foyer of the Queen Elizabeth building.
Orthopaedic Pre-Operative Assessment
Important information about your upcoming appointment:
Your appointment may last up to 2 hours and include blood sampling, an ECG, and an x-ray – please wear suitable clothing.
Please bring a list of all your medications.
Please bring reading glasses and hearing aids if you require them.
Please do not attend if you are unwell. Phone to re-arrange your appointment.
You are welcome to bring one family member/companion to the clinic.
If your health changes between this appointment and your surgery please let the nurses know.
Please note: If you are given a pre-op appointment it does not guarantee that you have a surgery date.
Glasgow Royal Infirmary
Telephone number for appointment queries: 0141 201 3721
There is a multi-story carpark within the hospital grounds (there is no charge for this carpark) There is multiple carparks around the hospital site, off High Street and on Wishart Street, these are private car parks and charge for parking.
Cafes/Canteens
The Little Royal Cafe (not NHS owned) is located next door to the Plastic Surgery Out Patient building, the hospital has 2 canteens, 1 situated in the Centre block and the Campsie restaurant in the basement of the Queen Elizabeth Building, there is an Aroma coffee shop within the main Foyer of the Queen Elizabeth building.
Anaesthesia allows you to be pain free and comfortable during your operation. For many operations this involves a general anaesthetic which is a state of controlled unconsciousness induced by medication. However, some modern anaesthetic techniques mean that this is not always required.
Spinal Anaesthesia is a technique by which the lower half of your body can be made completely numb. This means you can have a hip or knee replaced without a general anaesthetic. Most patients undergoing hip or knee replacement will have this type of anaesthetic when there are no surgical or medical reasons why it would not be suitable. Your preferences are also important and you will be able to discuss the options with your anaesthetist.
The benefits of a spinal anaesthetic are that, while you will be completely free of pain, you can remain fully conscious if you choose and listen to music (you are welcome to bring a portable music system and headphones with you) or doze off yourself so avoiding the sedative effects of medication. Equally, you may choose to have some sedation during the operation itself to help you relax or if you would prefer not to have clear memories of being in the surgical theatre. Your anaesthetist will discuss this with you on the day of surgery and ensure you are comfortable throughout.
The sensation and normal movement in your legs will return gradually after your operation allowing you to take timely pain relieving medication before the sensation has completely returned. This can help you manage the discomfort after the surgery. The risk of blood clots in your leg or bleeding may also be reduced. As with any anaesthetic or procedure there are potential side effects and complications. More detail regarding these and the other anaesthetic options that may be suitable are found in our Patient Consent leaflet for Hip and Knee Surgery.
In some cases, especially knee replacement surgery, your anaesthetist may place a longer lasting local anaesthetic around other nerves in your leg to help reduce the discomfort for a little longer after surgery. This is known as a “nerve block”. They will discuss this with you on the day of your operation.
There are occasions where, for medical or surgical reasons, a spinal anaesthetic is not suitable and your anaesthetist will be able to discuss the options with you. This often includes a general anaesthetic. Your preferences as to the type of anaesthetic you receive are also important so please take the time to consider these and ask your anaesthetist for advice. In some instances you may be asked to attend the hospital specifically to see an Anaesthetist if the specialist nursing staff in the pre-operative assessment clinic feel this would be of benefit to you. In most cases you will meet your Anaesthetist on the day of surgery.
Your anaesthetic for upper limb surgery
Hand and Foot Surgery – The Stobhill Block Room Journey
The ASPiRe programme supports people to prepare for surgery by promoting healthy behaviours and prescribing physical activity, nutrition and psychological interventions based on a person’s needs. This is called “prehabilitation”.
Here you will find information about what you can do and where you can find help to help you prepare for your operation and help your recovery.
NHS Scotland participation in the scheme created by The Redress for Survivors (Historical Child Abuse in Care) (Scotland) Act 2021.
On 6 December 2021, Scotland’s NHS Boards were formally invited to participate in the Redress Scheme for survivors of historical child abuse in residential care settings in Scotland.
We acknowledge the wrongfulness of historical child abuse, and the harm this caused to survivors. We offer our full and sincere apologies to anyone who suffered harm and abuse while in the care of NHS Scotland.
We recognise that this Scheme seeks to acknowledge and provide tangible recognition of past harm, and its impact on survivors. Participation in the Redress Scheme is a practical part of our national apology to children who suffered harm while in NHS care.
Further, we recognise that financial redress is only one aspect of acknowledging past harm within care settings for vulnerable children in Scotland.
All 22 of Scotland’s NHS Boards are fully committed to supporting the Redress Scheme. By contributing to the Scheme, we are setting out the commitment from NHS Scotland to support survivors and take steps to provide some redress for past trauma.
We therefore commit to living our values of care and compassion by pledging to be open, transparent and caring in how we engage with anyone who was in the care of NHS Scotland and who makes an application for a redress payment.
Information on the Scheme and support for people affected by this issue can be found through the following links:
This report sets out examples of wider (i.e., in addition to the redress scheme including non-financial) redress activities undertaken by NHS Scotland Health Boards from 7 December 2021 to 7 December 2022 as indicated in the Redress For Survivors (Historical Child Abuse In Care) (Scotland) Act 2021: Statutory Guidance.
Please see the consensus statement on metastatic surveillance of uveal melanoma in Scotland. This gives up to date information on how often we check your body for spread of eye melanoma.
The Molecular Radiotherapy (MRT) service offers a range of radionuclide therapies at Gartnavel General Hospital (GGH) and The Beatson West of Scotland Cancer Centre (BWoSCC) and is staffed by a friendly and professional multi-disciplinary team. The team includes medical doctors, technicians, nurses, physicists, healthcare support workers and clerical staff. Therapies take place in either Beatson main out patients, ward B3 or Nuclear medicine GGH.
Opening Times
Monday to Friday, 8.30am – 4.00pm (Closed Public Holidays & weekends)
Change / Cancel Appointment
If for any reason you are unable to attend your appointment, please inform us by telephoning 0141 301 7621 as soon as possible during office hours to contact your nurse specialist. We will make every effort to adjust your appointment.
Location
Therapies take place across multiple sites on the Gartnavel campus. Please see your patient info leaflet, which will come with your appointment, for location details.
Contact Details
Main nuclear medicine department number – 0141 301 7900
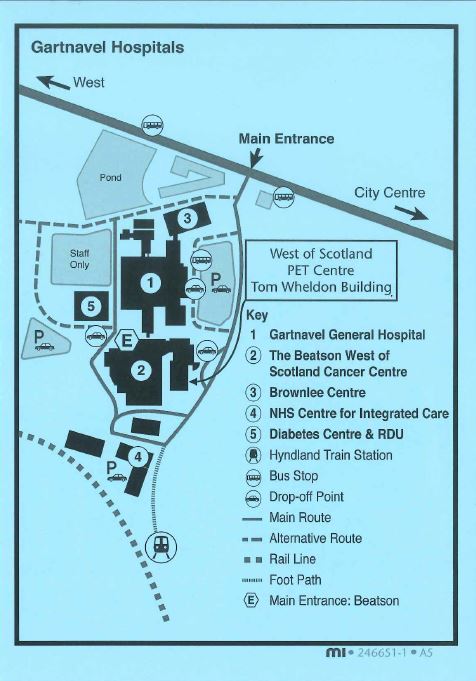
The Beatson West of Scotland PET centre is located on the Gartnavel Hospital Campus. If you have been referred for a PET-CT scan, we will post you an appointment letter, patient information leaflet and directions to the PET Centre. These should provide all the necessary information regarding where and when to attend, what preparation is required and answer many other questions you may have. However, should you have any further queries regarding your PET-CT scan, please call the department on 0141 301 7800 and staff will be happy to help.
Below is a video of what to expect when attending the department for a PET scan. Subtitles can be enabled in the settings menu at the bottom right of the video.
The West of Scotland PET Centre is on the Gartnavel Hospital Campus in the Tom Wheldon building of the Beatson Cancer Centre;
1053 Great Western Road, Glasgow, G12 0YN
Scottish Ambulance Service
The Scottish Ambulance Service has a central booking service which allows you to book ambulance transport. If you require this service, please phone 0300 123 1236 at least 3 days before your appointment but no sooner than 30 days in advance. Lines are open from 8.00am to 8.00pm Monday to Saturday.
Voluntary Hospital Transport Service
There are several options available if you require Hospital Transport Services to attend your appointment. Please see contacts below:
The Orthopaedic Research Department is situated in the Department of Orthopaedic Surgery at the Glasgow Royal Infirmary. We conduct a variety of clinical and basic research as well as exploring service redesign to improve the patient pathway through clinic.
Our clinical research portfolio revolves around the use of new robotic guided knee replacement surgeries to improve surgical accuracy, patient recovery and improve patient gait following knee replacement. We also assist in the recruitment of patients to trials that are centred outwith the Glasgow Royal Infirmary. Examples of these clinical trials can be found clicking the research link below.
As an active research department we frequently disseminate our research findings in journal articles. A list of these publications can be found via the publications link below.
If you would like more information on the research activities currently on-going in the Department or to discuss participating in an on-going clinical trial please contact: iii-ortho-research@glasgow.ac.uk
Permission to access patient records
We are seeking approval for permission to review the medical records of patients that took part in our two previous clinical trials, TRUCK and MAKO. This would involve seeking ethical approval to access patients’ medical records to record details of health care usage which is both related and un-related to their knee replacement. This is performed in an anonymised manner and only extracts information about how many times a participant has accessed a health care provider, with no details as to the reason for their visit. The aim of this new aspect of the study is to to review the participants retrospective NHS healthcare usage in a non-identifiable way to see if there is any downstream, long term differences between the patients who were randomised to receive the robotic-assisted knee surgery and conventional knee surgery groups. The difference in health care usage may highlight a potential cost benefit of the use of robotic or conventional surgery.
For access to the NHS Greater Glasgow and Clyde Data Privacy Notice, please follow the link below. This includes a section on data protection in Research and Innovation.
Information on upcoming projects and future collaborations, coming soon.
Upcoming Trials
Charity
Hip & Knee School
Was this helpful?
Yes
No
Thanks for your feedback!
Within the team there are many years of experience in orthopaedic nursing and the nursing staff have many specialist skills in caring for orthopaedic patients. In our department you will meet nurses trained in caring for you from your first visit, to pre-operative assessment and follow up.
Mairi MacKinnon is the Limb Reconstruction Clinical Nurse Specialist based at Glasgow Royal Infirmary. She has recently joined the limb reconstruction team having previously served within the orthopaedic department as the musculoskeletal oncology nurse specialist for over 2 years.
Mairi manages all limb reconstruction patients including patients with external fixators, in particular, circular frames. She also assists the Intramedullary Nail Clinic where all tibial patients attend for review. As part of her role within the limb reconstruction service, she manages complex surgical wounds and has extensive experience in Negative Pressure Wound Therapy.
Pamela McKirdy is a Staff Nurse in the Orthopaedic Outpatients Department. She has worked in Orthopaedic Outpatients for 24 years gaining a wealth of experience and knowledge in Orthopaedic conditions, trauma and elective surgeries and wound care. She has completed the casting course and has specialist training and experience in managing both elective and trauma surgeries post-operatively and on many occasions it may be Pamela who will review your condition or surgery in a stand-alone clinic where your entire care will be managed by experienced nurses and your x-rays reviewed. She is able to consult directly with senior medical staff if appropriate regarding any unusual findings.
Sarah Vaughan – Oncology Clinical Nurse Specialist
Sarah is the Clinical Nurse Specialist for the Musculoskeletal Sarcoma Oncology Service based at Glasgow Royal Infirmary. Sarah recently joined the team having previously worked as an Oncology Clinical Nurse Specialist for 6 years within another Trust.
The Oncology team form part of a specialist service who have extensive knowledge and expertise in managing Sarcoma. This team provides a comprehensive service that covers investigation of suspected disease, diagnosis, treatment and follow-up.
It’s Sarah’s job to provide support throughout this time, offering advice and a point of contact whilst patients undergo investigations and/or treatment.
We use cookies to analyse traffic to our site and to enable certain functions such as forms and embedded videos. These do not collect personal information. By clicking "Accept All", you consent to our use of cookies, or you can customise the options.
This website uses cookies
Websites store cookies to enhance functionality and personalise your experience. You can manage your preferences, but blocking some cookies may impact site performance and services.
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
CloudFlare provides web performance and security solutions, enhancing site speed and protecting against threats.
Sequence rules uses cookies to track the order of requests a user has made and the time between requests and makes them available via Cloudflare Rules. This allows you to write rules that match valid or invalid sequences. The specific cookies used to validate sequences are called sequence cookies.
session
cf_ob_info
The cf_ob_info cookie provides information on: The HTTP Status Code returned by the origin web server. The Ray ID of the original failed request. The data center serving the traffic
session
cf_chl_rc_m
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
__cfruid
Used by the content network, Cloudflare, to identify trusted web traffic.
session
__cf_bm
Cloudflare's bot products identify and mitigate automated traffic to protect your site from bad bots. Cloudflare places the __cf_bm cookie on End User devices that access Customer sites that are protected by Bot Management or Bot Fight Mode. The __cf_bm cookie is necessary for the proper functioning of these bot solutions.
session
__cflb
When enabling session affinity with Cloudflare Load Balancer, Cloudflare sets a __cflb cookie with a unique value on the first response to the requesting client. Cloudflare routes future requests to the same origin, optimizing network resource usage. In the event of a failover, Cloudflare sets a new __cflb cookie to direct future requests to the failover pool.
session
_cfuvid
The _cfuvid cookie is only set when a site uses this option in a Rate Limiting Rule, and is only used to allow the Cloudflare WAF to distinguish individual users who share the same IP address.
session
cf_clearance
Whether a CAPTCHA or Javascript challenge has been solved.
session
cf_use_ob
The cf_use_ob cookie informs Cloudflare to fetch the requested resource from the Always Online cache on the designated port. Applicable values are: 0, 80, and 443. The cf_ob_info and cf_use_ob cookies are persistent cookies that expire after 30 seconds.
session
__cfwaitingroom
The __cfwaitingroom cookie is only used to track visitors that access a waiting room enabled host and path combination for a zone. Visitors using a browser that does not accept cookies cannot visit the host and path combination while the waiting room is active.
session
cf_chl_rc_i
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
cf_chl_rc_ni
These cookies are for internal use which allows Cloudflare to identify production issues on clients.
session
Statistics cookies collect information anonymously. This information helps us understand how visitors use our website.
We use Microsoft Clarity to understand how users interact with our website, including information such as clicks, scrolling and navigation behaviour, to help improve our services.
Microsoft Clarity uses cookies and similar technologies. These are only set if you accept analytics cookies.
If you choose not to accept analytics cookies, Clarity will operate in a limited mode using non-cookie-based data, which does not track users across pages or visits.
The data collected is behavioural and technical in nature and does not directly identify individuals. Sensitive information such as names, email addresses and form inputs is automatically hidden and not recorded or viewed.
Some information, such as device and approximate location data will still be collected and is treated as personal data in accordance with data protection legislation.
This will not be used for any purpose other than analytics and will not be used to identify you.
We use Microsoft Clarity to understand how users interact with our website, including information such as clicks, scrolling and navigation behaviour, to help improve our services.
Microsoft Clarity uses cookies and similar technologies. These are only set if you accept analytics cookies.
If you choose not to accept analytics cookies, Clarity will operate in a limited mode using non-cookie-based data, which does not track users across pages or visits.
The data collected is behavioural and technical in nature and does not directly identify individuals. Sensitive information such as names, email addresses and form inputs is automatically hidden and not recorded or viewed.
Some information, such as device and approximate location data will still be collected and is treated as personal data in accordance with data protection legislation.
This will not be used for any purpose other than analytics and will not be used to identify you.